
Native American disease and epidemics
The examples and perspective in this article may not represent a worldwide view of the subject. (July 2016) |
This article may lend undue weight to certain ideas, incidents, or controversies. (July 2016) |
Native American disease and epidemics pervade many aspects of Native American life, both throughout history and in the present day. Diseases and epidemics can be chronicled from centuries ago when European settlers brought diseases that devastated entire tribes to the modern day when Native Americans face serious struggles with particular diseases. The current crises in diseases and epidemics are addressed by many different groups, both governmental and independent, through a multitude of programs.
European contact

The arrival of Europeans ushered in what is termed the Columbian Exchange. During this period European settlers brought many different technologies and lifestyles with them; arguably the most harmful effect of this exchange was the arrival and spread of disease.[1]
Native Americans, due to the lack of prior contact with Europeans, had not previously been exposed to the diseases that were prevalent on the distant continent. Therefore, they had not built up internal immunities to the diseases or formed any medicines to combat them. Europeans came into the New World bearing various diseases. Those infected with diseases either possessed them in a dormant state or were not quarantined in such a way that distanced them enough from Native Americans not to spread the diseases, allowing them to spread into epidemics.[1]
The diseases brought by Europeans are not easily tracked, since there were numerous outbreaks and all were not equally recorded. The most notable disease brought by Europeans was smallpox. The Lakota Indians called the disease the running face sickness.[2] Smallpox was lethal to many Native Americans, bringing sweeping epidemics and affecting the same tribes repeatedly. In the summer of 1639, a smallpox epidemic struck the Huron natives in the St. Lawrence and Great Lakes regions. The disease had reached the Huron tribes through traders returning from Québec and remained in the region throughout the winter. When the epidemic was over, the Huron population had been reduced to roughly 9000 people, about half of what it had been before 1634.[3] Between 1837 and 1870, at least four different epidemics struck the Plains tribes.[4] When the plains Indians began to learn of the "white man’s diseases", they intentionally avoided contact with them and their trade goods. But many tribes were enamored with things like metal pots, skillets and knives, and they traded with the white newcomer anyway, inadvertently spreading diseases to their villages.[2]
Numerous other diseases were brought to North America, including measles, scarlet fever, typhoid, typhus, influenza, pertussis (whooping cough), tuberculosis, cholera, diphtheria, chickenpox, the common cold, and sexually transmitted diseases.[4][5] Each of these brought destruction through sweeping epidemics, involving illness and extensive deaths. Many Native American tribes experienced great depopulation, averaging 25–50 percent of the tribes members lost to disease. Additionally, smaller tribes neared extinction after facing severely a destructive spread of disease.[4] The significant toll that this took is expounded upon in the article Population history of indigenous peoples of the Americas. A specific example was Cortes' invasion of Mexico. Before his arrival, the Mexican population is estimated to have been around 25 to 30 million. Fifty years later, the Mexican population was reduced to 3 million, mainly by infectious disease. This shows the main effect of the arrival of Europeans in the new world. With no natural immunity against these pathogens, Native Americans died in huge numbers. The eminent Yale historian David Brion Davis describes this as "the greatest genocide in the history of man. Yet it's increasingly clear that most of the carnage had nothing to do with European barbarism. The worst of the suffering was caused not by swords or guns but by germs”.[6]
Certain cultural and biological traits made Native Americans more susceptible to these diseases. Emphasis placed on visiting the sick led to the spread of disease through consistent contact.[7] Smallpox specifically led indirectly to higher rates of suicide. Many Native American tribes prided themselves in their appearance, and the resulting skin disfigurement of smallpox deeply affected them psychologically. Unable to cope with this psychological development, tribe members were said to have committed suicide.[8]
Native Americans first exposed to these diseases also had a unique approach to illness, relating primarily to religious beliefs. There is the belief that disease is caused by either a lack of charm use, an intrusion of an object by means of sorcery, or the free soul's absence from the body. Disease was understood to enter the body if one is not protected by the spirits, as it is a natural occurrence. Religious powers were believed to be related to curing diseases as well.[9] Native American illness has been treated through the practice of shamanism in the past, though this decreased as the influence of Europeans increased.
Disease evolution and host pathogen interactions should be considered in Native American disease history. Disease evolution is the result of the interaction of the following parameters: hosts, parasites, and setting. Such an example of disease evolution is the direct biological effects of crowding that directly influences a host’s susceptibility to disease. Research by Power et al. (1998) demonstrated that, at low doses of micro-bacterial pathogens, hosts were able to make an appropriate immune response and avoid tuberculosis; higher doses resulted in a less efficient form of a vaccination. The crowding that was a result of widespread relocation and concentration of native groups by the expanding America greatly impacted the susceptibility native people initially had to the foreign diseases.[10]
Disease as a weapon against Native Americans
"You will do well to try to inoculate the Indians, by means of blankets, as well as to try every other method that can serve to extirpate this execrable race." — Jeffery Amherst[11]
The spread of disease from European contact was not always accidental. Europeans arriving in the Americas had long been exposed to the diseases, attaining a measure of immunity, and thus were not as severely affected by them. Therefore, disease could be an effective technique as a biological.[11]
During the French and Indian War, Jeffery Amherst, 1st Baron Amherst, Britain's commander in chief in North America suggested using smallpox to wipe out their Native American enemy. In his writings to Colonel Henry Bouquet about the situation in western Pennsylvania,[11] Amherst suggested that the spread of disease would be beneficial in achieving their aims. Colonel Bouquet confirmed his intentions to do so.
Biological warfare during the Siege of Fort Pitt
"Out of our regard to them we gave them two Blankets and an Handkerchief out of the Small Pox Hospital. I hope it will have the desired effect."
This event is well known for the documented instances of biological warfare. British officers, including the top British commanding generals, ordered, sanctioned, paid for and conducted the use of smallpox against the Native Americans. As described by one historian, "there is no doubt that British military authorities approved of attempts to spread smallpox among the enemy", and "it was deliberate British policy to infect the indians with smallpox".[12]
In this instance, as recorded in his journal by sundries trader and militia Captain, William Trent, on June 24, 1763, dignitaries from the Delaware tribe met with Fort Pitt officials, warned them of "great numbers of Indians" coming to attack the fort, and pleaded with them to leave the fort while there was still time. But the commander of the fort refused to abandon the fort. Instead, the British gave as gifts two blankets, one silk handkerchief and one linen from the smallpox hospital,[13] to two Delaware delegates after the parley, a principal warrior named Turtleheart, and Maumaultee, a Chief. The tainted gifts were, according to their inventory accounts, given to the Indian dignitaries "to Convey the Smallpox to the Indians".[14][15]
Levy, Trent and Company: Account against the Crown, Aug. 13, 1763[13]
"To Sundries got to Replace in kind those which were taken from people in the Hospital to Convey the Smallpox to the Indians Vizt:
2 Blankets @ 20/ £299 099 0
1 Silk Handkerchef 10/
& 1 linnen do: 3/6 099 1399 6
Captain Ecuyer later certified that the items "were had for the uses above mentioned," in the inventory reimbursement request, and General Thomas Gage would later approve that invoice for payment, endorsing it with a comment and his signature.[13]
While Ecuyer, Trent and McKee were conducting their early form of biological warfare upon the Indian dignitaries at Fort Pitt, their superiors were discussing similar plans. General Amherst, having learned that smallpox had broken out among the garrison at Fort Pitt, and after learning on July 7 of the loss of his forts at Venango, Le Boeuf and Presqu'Isle, wrote to Colonel Bouquet, "Could it not be contrived to send the small pox among the disaffected tribes of Indians? We must on this occasion use every stratagem in our power to reduce them." In addition, Amherst wrote, "Captain Ecuyer Seems to Act with great Prudence, & I approve of everything he mentions to have done." Bouquet, who was already marching to relieve Fort Pitt and Fort Detroit, responded on the 13th, "I will try to inoculate the Indians with some blankets that may fall into their hands, and take care not to get the disease myself. I wish we could make use of the Spanish method to hunt them with English dogs, supported by rangers and some light horse, who would, I think, effectually extirpate or remove that vermin." On July 16, Amherst replied, "You will do well to try to inoculate the Indians by means of blankets, as well as to try every other method that can serve to extirpate this execrable race. I should be very glad your scheme for hunting them down by dogs could take effect, but England is at too great a distance to think of that at present."[16]
General Amherst, July 8: "Could it not be contrived to Send the Small Pox among those Disaffected Tribes of Indians? We must, on this occasion, Use Every Stratagem in our power to Reduce them."
Colonel Bouquet, July 13: "I will try to inocculate the Indians by means of Blankets that may fall in their hands, taking care however not to get the disease myself."
Amherst, July 16: "You will Do well to try to Innoculate the Indians by means of Blanketts, as well as to try Every other method that can serve to Extirpate this Execreble Race."
Bouquet, July 19: "all your Directions will be observed."
The correspondence between Amherst and Bouquet reflected how pervasive Indian hating had become by 1763 and how far British officers were willing to go in ignoring their own soldiers' code of warfare.[16] A devastating smallpox epidemic plagued Native American tribes in the Ohio Valley and Great Lakes area through 1763 and 1764, but the effectiveness of individual instances of biological warfare remains unknown. After extensive review of surviving documentary evidence, historian Francis Jennings concluded the attempt at biological warfare was "unquestionably effective at Fort Pitt";[17] Barbara Mann deduced "it is important to note that the smallpox distribution worked";[18] Howard Peckham noted the resulting fatal epidemic "certainly affected their vigorous prosecution of the war."[14]
Dissent against the history of biological weapon usage
There has been some dissent to the accepted history that certain outbreaks of smallpox were caused by the intentional spreading of disease, for example when smallpox-infested blankets were intentionally given to Native Americans in 1763 at the Siege of Fort Pitt. Nineteenth century historian Francis Parkman, the first to research these events, described "the shameful plan of infecting the Indians" as "detestable."[19] It is likely such incidents have occurred more frequently than scholars have acknowledged, but with such actions considered beyond the pale of civilized behavior, incriminating documentation would be scarce. Efforts have ever since been made to reduce the stigma associated with being the perpetrators of such acts.[13][20] Captain Ecuyer's official report, written at the time of the incident and in great detail, notably did not mention the tainted gifts. According to biological warfare expert Mark Wheelis, Ecuyer considered concealing the event and acknowledged the deed in his ledgers only after learning that his superiors were ordering the same course of action.[21] The most widely cited expert on the subject, Elizabeth Fenn, has observed, "It is also possible that documents relating to such a plan were deliberately destroyed."[13] Peckham noted that, "oddly enough", the incriminating pages from Amherst and Bouquet were missing from the Canadian Archives transcripts as well as the collection published by the Pennsylvania Historical Commission.[14] Likewise, Mann has described documents which have gone missing after "later sanitation", and has documented efforts by "Amherst apologists" and others who conjecture about, minimize and even dispute the instances of European perfidy. One historian says that though blankets containing smallpox were distributed to Native Americans by the Europeans, they may have been given with good will and intentions, instead of for the purpose of disseminating disease, contrary to what was recorded in the trade ledgers. Additionally, scholars such as Gregory Dowd, are of the opinion that disease was also spread by Native Americans returning from battling infected Europeans, and therefore it may also have been spread by Native Americans to their own people.[22] Dixon has suggested that the attempt to infect the Indians near Fort Pitt "may well have been a failure",[12] and Ranlet has speculated that "either the smallpox virus was already dead on the unpleasant gifts or that the presents simply failed to fulfill Trent's ardent desire to infect the Indians."[23] Mann has called such assumptions "demonstrably false", and Wheelis has concluded that while there may have been several simultaneous routes of transmission for the epidemic, and the effect of each attempt is impossible to determine, "the act of biological aggression at Fort Pitt is indisputable".[21]
Effects of smallpox on the native peoples
These foreign diseases were a constant threat to the native peoples of the Americas. A preponderance of documented evidence suggests that smallpox has plagued natives for many years prior to, and after the Fort Pitt exchange. The exact level of success of the attempt to "inoculate" the native tribes in the area by giving tainted objects to their dignitaries Turtle's Heart and Mamaltee,[24] is unknown. Thomas Hutchins, in his August 1762 Journal entry among the Natives at Fort "Mineamie", reports: "The 20th, The above Indians met, and the Ouiatanon Chief spoke in behalf of his and the Kickaupoo Nations as follows: '"Brother, We are very thankful to Sir William Johnson for sending you to enquire into the State of the Indians. We assure you we are Rendered very miserable at Present on Account of a Severe Sickness that has seiz'd almost all our People, many of which have died lately, and many more likely to Die." Later, Hutchins writes "The 30th, Set out for the Lower Shawneese Town' and arriv'd 8th of September in the afternoon. I could not have a meeting with the Shawneese untill the 12th, as their People were Sick and Dying every day."[25]
Gershom Hicks, taken captive in May 1763 by the Shawnee and Delaware, reported that an epidemic was underway among the natives in the spring of 1763 and well into 1764. Hicks escaped and arrived to Fort Pitt on April 14, 1764. He reported to the 42nd Regiment Captain William Grant "that the Small pox has been very general & raging amongst the Indians since last spring and that 30 or 40 Mingoes, as many Delawares and some Shawneese Died all of the Small pox since that time, that it still continues amongst them."[26]
John McCullough, a Delaware captive since July, 1756, who was then 15 years old, wrote: "Soon after we got home to Mahoning, instead of taking me to Pittsburgh, agreeable to their promise, they set out on their Fall hunt, taking me along with them; we staid out till some time in the Winter before we returned" He continues that, on June 2, 1763,[27][28] "Shortly after the commencement of the war, they plundered a tanyard near to Pittsburgh, and carried away several horse-loads of leather;",[27][29] and recalled that, beginning on July 5th, 1763,[30] the Lenape people, under the leadership of Shamokin Daniel, "committed several depredations along the Juniata; it happened to be at a time when the smallpox was in the settlement where they were murdering, the consequence was, a number of them got infected, and some died before they got home, others shortly after; those who took it after their return, were immediately moved out of the town, and put under the care of one who had the disease before."[31][32]
Mary Jemison, a Seneca captive, was taken in 1755 in what is now Adams County, Pennsylvania. She married a Delaware, and later chose to remain with the Seneca. In James E. Seaver's (Jemison's biographer) interview, she described her many hardships, including travels to Fort Pitt. In 1762, her seventh year of captivity, she reported the death of her first husband from "sickness".[33]
Contemporary diseases
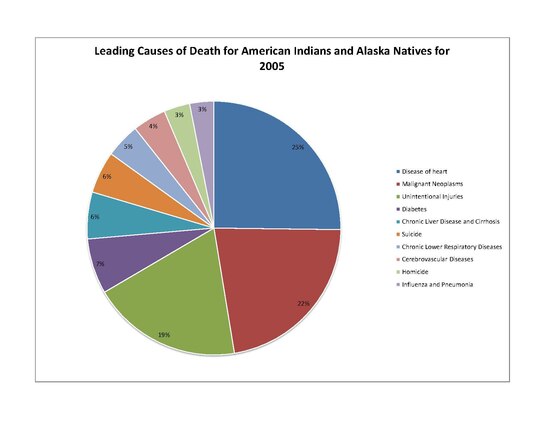
Currently, Native Americans share many of the same health concerns as their non-Native American, United States citizen counterparts. For instance, Native Americans leading causes of death include "heart disease, cancer, unintentional injuries (accidents), diabetes, and stroke." Other health concerns include "high prevalence and risk factors for mental health and suicide, obesity, substance abuse, sudden infant death syndrome (SIDS), teenage pregnancy, liver disease, and hepatitis." Diseases primarily present the greatest threat to Native American life. The top leading causes of death include the following diseases: heart disease, cancer, diabetes, and chronic liver disease / cirrhosis.[34][35]
Though many of these appear to be concerns paralleling those of non-Native Americans, some of these diseases present a much greater threat to Native Americans' well-being.[36] These discrepancies in disease patterns vary significantly between diseases, but have a notable impact on the population. There are many general reasons for the discrepancies in Native American disease prevalence.[37]
The genetic composition of Native Americans and clans can have an influence on many diseases and their continuing presence. The commonly lower socioeconomic status limits the ability of many to receive adequate health care and make use of preventative measures. Also, certain behaviors that take place commonly in the Native American culture can increase risk of disease.[37] When the period of tribal termination in the 20th century occurred, pot termination many tribes could no longer afford to keep their hospitals open.[38]
Native Americans have much higher smoking rates than the white, black, and Asian demographics. Native American men are about as likely to be moderate to heavy drinkers as white men, but about 5–15% more likely to be moderate to heavy drinkers than black or Asian men. Native Americans are 10% less likely to be at a healthy weight than white adults, and 30% less likely to be at a healthy weight than Asian adults. On a similar note, they have far greater rates of obesity, and were also less likely to engage in regular physical activity than white adults.[39]
Data collected by means of secondary sources such as the US Census Bureau and the Centers for Disease Control and Prevention's National Center for Health Statistics showed that from 1999-2009 Alaska Natives and Native Americans had high mortality rates to infectious diseases when compared to the mortality rate of white Americans. Alaska natives from the age groups 0-19 and 20-49 had death rates 4 to 5 times higher than compared to whites. Native Americans from the 20-49 age group in the Northern Plains were also 4 to 5 times more likely to die to infectious diseases than whites. Also found was that American Indians and Alaska Natives were 13 times more likely to contract tuberculosis than whites.
American Indian or Alaska Native were at least twice as likely to have unmet medical needs due to cost and were much less likely to have seen a dentist within the last 5 years compared with white or Asian adults, putting them at risk for gingivitis and other oral diseases. As it stands, American Indian/ Alaska Natives face high rates of health disparity compared to other ethnic groups.[40]
Heart disease
The leading cause of death of Native Americans is heart disease. In 2005, it claimed 2,659 Native American lives. Heart disease is notable in Native American populations because it occurs at a rate 20 percent greater than all other United States races. Additionally, the demographic of Native Americans who die from heart disease is younger than other United States races, with 36% dying of heart disease before age 65.[41] The highest heart disease death rates are located primarily in South Dakota and North Dakota, Wisconsin, and Michigan.[42]
Heart disease in Native Americans is not only due to diabetic complications; the increased risk is also due to higher rates of hypertension. Native American populations have been documented as being more likely to have high blood pressure than other groups, such as white Caucasians.[43] Studies have also been conducted that associate the exposure to stress and trauma to an increased rate of heart disease. It has been documented in Native American populations that adverse childhood experiences, which are significantly more common in the Native American demographic, have a positively linear relationship with heart disease, as well an increasing influence on symptoms of heart disease.[44]
Cancer
Cancer has a documented presence amongst Native Americans, and the rates of certain types of cancer exceed that of the general population of the United States. For instance, Native American males were twice as likely to have liver cancer than white males from 2001–05. Women on the other hand are 2.4 times as likely to have and die from liver cancer as their white counterparts. This has a notable correlation with the rates of alcoholism of Native Americans, which are greater than the general population.[45]
Stomach cancer was also 1.8 times more common in Native American males than white males, in addition to being twice as likely to be fatal. Other cancers, such as kidney cancer, are more common among Native American populations. It is important to note that overall cancer rates are lower among Native Americans compared to the white population of the United States. For cancers that are more prevalent in Native Americans than the white United States population, death rates are higher.[45]
Diabetes

Diabetes has posed a significant health risk to Native Americans. Type I diabetes does not have a notable correlation to Native Americans, and is rather rare. Type II diabetes is a much more significant problem and is the type of diabetes referred to in the remainder of this section. The prevalence of diabetes began primarily in the middle of the twentieth century and has grown into an epidemic. About 16.3% of Native American adults have been diagnosed with diabetes.[46] Type two diabetes and the complications that follow have gone from being acute infectious diseases to chronic illnesses within American Indian and Alaska Native communities. American Indians and Alaska Natives experience high rates of end-stage renal disease, which is mainly driven by, and directly correlates with, the increase in diabetes within their communities.[47]
Native Americans are about 2.8 times more likely to have Type II diabetes than white individuals of comparable age. The rates of diabetes among Native Americans also continue to rise. During the eight-year span of 1990 to 1998, diabetes grew 65% among the Native American population. This is very significant growth, and this growth continues in the present day. [48]
The highest rates of diabetes in the world are also found among a Native American tribe. The Pima tribe of Arizona took part in a research study on diabetes which documented diabetes rates within the tribe. This study found that the Pimas had diabetes rates 13 times that of population of Rochester, Minnesota, a primarily white populace. Diabetes was documented in over one third of Pimas from ages 35–44, and in over sixty percent of those over 45 years of age.[49]
There are multiple causes for diabetes to cast such a presence on the Native American demographic:
- Genetic Predisposition
- Native Americans with the "least genetic admixture with other groups"[48] have been found to be at a higher risk of developing diabetes, showing that this minority group has a great predisposition for diabetes which increases the risk of its contraction
- Obesity
- Native Americans have a significant health problem with obesity, as they are 1.6 times more likely to be obese than a white American.;[36] Native Americans are as likely as black adults to be obese.[40] Obesity is known as a general causative factor of diabetes, which is generally caused by Food Deserts, a lack of readily available nutritious foods, in reservations.
- Low Birth Weight
- The notable association between low birth weight and increased risk in diabetes has been documented in Native American populations[48]
- Diet
- Changes in Native American diets have been associated with the increase in diabetes, as more high calorie and high fat foods are consumed, replacing the traditionally agriculturally driven diet.[50] As time has gone there has been a push for Native Americans to return to their traditional ways; including growing and eating traditional foods. The Centers for Disease Control and Prevention (CDC) has been a huge proponent of Native Americans returning to traditional diets. Even going as far as too make a PSA in 2013, which involved Cherokee actors discussing diabetes, and the impact diet has on their increased risk.[51]
Mental health
Other issues that Native Americans are facing are things like mental health and suicide. Native Americans have the highest rate of suicide out of any ethnic group in the United States, in 2009 suicide was the leading cause of death among Native Americans and Native Alaskans between the ages of 10 and 34.[52] 75% of deaths among Native Americans and Native Alaskans over the age of 10 are due to unintentional injury, homicide, and suicide.[52] Suicide rates among Native American youths is significantly higher than the suicide rates among white youths.[52] The head of the IHS, Mary L. Smith, says[when?] that there will be a new focus on mental health issues in American Indian communities, and that since there is a tremendous amount of suicide among teens on the Pine Ridge reservation they are designating it a Promise Zone and sending extra help.[53] Native people's mental health is also effected by being stigmatized as drunks the media in movies and, which negatively impacts their mental health and self-esteem. Potentially, If native people are constantly told that they are drunks, some may just accept that this is all society will see of them and gives into depression and alcoholism. Native children are not given role models in movies or TV to look up to, which impacts what they believe possible for their futures.[54]
Impact
Along with this significant presence of diabetes comes the notable presence of complications, such as end-stage renal disease.[47] Each of these are more prevalent in the Native American population.[55] Diabetes has been seen to cause premature death of Native Americans by vascular disease, more notably in those diagnosed with diabetes later in life. It has been reported among the Pima Indians to cause elevated urinary albumin excretion. Native Americans with diabetes have a significantly higher rate of heart disease than those without diabetes, and cardiovascular disease is the "leading underlying cause of death in diabetic adults" in Native Americans.[50]
Diabetes has caused nephropathy among Native Americans, leading to renal function deterioration, failure, and disease. Prior to the increase in cardiovascular disease among diabetic Native Americans, renal disease was the leading cause of death. Another complication documented in diabetic Native Americans, as well as other diabetic populations, is retinopathy.[50]
Lower extremity amputations are also notably higher among Native American populations with diabetes. In studies of the Pima Indians, those with diabetes were found to have much higher prevalence of periodontal disease. Additionally, those with diabetes have higher instances of bacterial and fungal infection. This is seen in statistics such as "diabetic Sioux (Lakota people) Indians were four times as likely to have tuberculosis as those without diabetes."[50]
With such alarming numbers of type II diabetes it is important to understand how the Native American population got to this point and see if there are any trends in common with the world situation today. Prior to the 1940s diabetes was virtually unheard of, but ever since the 1960s the prevalence has been on the rise. This rise is thought to be in part due to their food history and culture. Native Americans had a diverse food history prior to colonization, but after colonization the natives were forced to live on non-traditional lands and eat government hand-outs for food. Much of this food was of low quality, meaning that here is not much nutritional content for the caloric intake and led to many Natives being malnourished.
It is important to note that Native Americans with diabetes have a death rate three times higher than those in the non-Native population. Diabetes can shorten a person's life by approximately 15 years.[46] As of 2012, diabetes was not the leading cause of death for Native Americans itself but contributed significantly to the top leading causes of death.[34]
The enormous barriers for Native Americans and Alaskan Natives to receive proper health care should also be considered when looking at the impact of medical afflictions Native Americans go through. Such barriers include but are not limited to: the isolated locations of some tribes make traveling to facilities far too difficult to travel the distance, hazardous roads, high rates of poverty mean less access to healthcare and means of transportation to get said health care, and too little staff in hospitals near reservations combined with the high numbers of patients with diabetes and extrarenal diabetic complications results in less availability for proper treatment. Another contributing factor is that Native people generally wait longer for organ transplants than white people. Diabetes is primary cause of end-stage renal disease, and dialysis treatments and kidney transplants remain the most effective methods of treatment[47]
Alcoholism
Another significant concern in Native American health is alcoholism. Alcoholism in the modern day is approached as a disease, and has been strongly linked to genetics and social circumstances. The rate of death from alcoholism in Native Americans is about five times that of all races in the United States.[56] However, due to the nature of alcoholism and the behaviors involved, the disease model is not always applicable. It is clearly a disorder that has many factors, but the behavioral component distinguishes it from many other diseases, such as those previously discussed.[57] Alcoholism, along with drug use, is discussed in Modern social statistics of Native Americans. However, In contrast to enduring and often racist stories about extraordinarily high rates of alcohol abuse among Native Americans, University of Arizona researchers have found that Native Americans’ binge and heavy drinking rates actually match those of whites. The groups differed regarding abstinence: Native Americans were more likely to abstain from alcohol use.
The “Drunken Indian” myth, perpetuates a stereotype that affects everything from the kind of jobs a native person gets, to the kind of diagnosis that a doctor gives a native person.[58]
From the National Survey on Drug Use and Health (spanning from 2009 to 2013 which included data from more than 4,000 Native Americans and 170,000 whites), and The Behavioral Risk Factor Surveillance System survey (conducted between 2011 and 2013, covered more than 21,000 Native Americans and 1 million whites) about 17 percent of whites and Native Americans were binge drinkers. When asked about the last time they had a drink, 40% percent of Native Americans had a drink during the previous month, compared to 43 percent of whites who did consume alcohol in the previous month. Despite only drinking marginally less than white people, Native Americans may be more vulnerable to the risks associated with drinking because of other issues, such as a lack of access to health care, safe housing and clean water[58]
HIV/AIDS
HIV and AIDS are growing concerns for the Native American population. The overall percentage of Native Americans diagnosed with either HIV or AIDS within the entire United States population is relatively small, but noting the percentage of the population that is Native American this is a notable figure. Native American AIDS cases make up approximately 0.5% of the nation's cases, while they account for about 1.5% of the total population.[36]
Native Americans and Alaska Natives rank third in the United States in the rate of new HIV infections.[59] Also notable is the fact that Native Americans, when counted with Alaskan Natives, have a 40% higher rate of AIDS than white individuals. Also, Native American and Alaskan Native women have double the rate of AIDS of white women.[36]
These statistics have multiple suggested causes:
- Sexual behaviors
- Previous studies of high rates of sexually transmitted diseases among Native Americans lead to the conclusion that the sexual tendencies of Native Americans lead to greater transmission[60]
- Illicit drug use
- The use of illicit drugs is documented to be very high among Native Americans, and not only does the involvement of individuals with illicit drugs correlate with greater rates of sexually transmitted disease, but it can facilitate the spread of diseases
- Socio-economic status
- Due to the poverty and lower rates of education, the risk of getting AIDS or any other sexually transmitted disease can be increased indirectly or directly
- Testing and data collection
- Native Americans may have limited access to testing for HIV/AIDS due to location away from certain health facilities; data collected on Native American sexually transmitted diseases may be limited for this same reason as well as for under reporting and the Native American race being misclassified[60]
- Culture and tradition
- Native American culture is not always welcoming of open discussion of sexually transmitted diseases[59]
Stroke
Other diseases pose notable concerns to the Native American demographic as well. Stroke is the sixth leading cause of death in the Native American population. Native Americans are sixty percent more likely than white adults in the United States to have a stroke. Native American women have double the rate of stroke of white women. About 3.6% of Native American and Alaska Native men and women over 18 have a stroke.[61] The stroke death rate of Native Americans and Alaska Natives is 14 percent greater than among all races.[62]
Combating disease and epidemics
Many initiatives have been put in place to combat Native American disease and improve the overall health of this demographic. One primary example of such initiative by the government is the Indian Health Service which works "to assure that comprehensive, culturally acceptable personal and public health services are available and accessible to American Indian and Alaska Native people."[63] There are many other governmental divisions and funding for health care programs relating to Native American diseases, as well as a multitude of programs administered by tribes themselves.
Diabetes programs

As diabetes is one of the utmost concerns of the Native American population, many programs have been initiated to combat this disease. In some native communities.
Governmental programs
One such initviative has been developed by the Centers for Disease Control and Prevention (CDC). Termed the "Native Diabetes Wellness Program", this program began in 2004 with the vision of an "Indian Country free of the devastation of diabetes."[64] To realize this vision, the program works with Native American communities, governmental health institutions, other divisions of the CDC, and additional outside partners. Together they develop health programs and community efforts to combat health inequalities and in turn prevent diabetes. The four main goals of the Native Diabetes Wellness Program are to promote general health in Native communities (physical activity, traditional foods), spread narratives of traditional health and survival in all aspects of life, utilize and evaluate health programs and education, and promote productive interaction with the state and federal governments.[64]
Funding for these efforts are provided by the Balance Budget Act of 1997, Public Law 105-33, and the Indian Health Service. One successful effort of this program is the Eagle Books series, which are books using animals as characters to depict a healthy lifestyle that prevents diabetes, including embracing physical activity and healthy food. These books were written by Georgia Perez, who worked with the University of New Mexico’s Native American Diabetes Project.[65] Other successful efforts include Diabetes Talking Circles to address diabetes and share a healthy living message and education in schools. The Native Diabetes Wellness Program also has worked with tribes to establish food programs that support the "use of traditional foods and sustainable ecological approaches"[64] to prevent diabetes.
The Indian Health Service has also worked to control the diabetes prevalence among Native Americans. The IHS National Diabetes Program was created in 1979 in order to combat the escalating diabetes epidemic.[66] The current head of the IHS is Mary L. Smith, Cherokee, took the position in March 2016 and has pledged to improve the IHS and focus on comprehensive health care for all the tribes and people covered by the department.[53] A sector of the service is the Division of Diabetes Treatment and Prevention, which "is responsible for developing, documenting, and sustaining clinical and public health efforts to treat and prevent diabetes in American Indians and Alaska Natives."[66]
This division contains the Special Diabetes Program for Indians, as created by 1997 Congressional legislation. This program receives $150 million a year in order to work on "Community-Directed Diabetes Programs, Demonstration Projects, and strengthening the diabetes data infrastructure."[66] The Community-Directed Diabetes Programs are programs designed specifically for Native American community needs to intervene in order to prevent and treat diabetes. Demonstration Projects "use the latest scientific findings and demonstrate new approaches to address diabetes prevention and cardiovascular risk reduction."[66] Strengthening the diabetes data infrastructure is an effort to attain a greater base of health information, specifically for the IHS Electronic Health Record.[66]
In addition to the Special Diabetes Program for Indians, the IHS combats diabetes with Model Diabetes Programs and the Integrated Diabetes Education Recognition Program. There are 19 Model Diabetes Programs which work to "develop effective approaches to diabetes care, provide diabetes education, and translate and develop new approaches to diabetes control."[66] The Integrated Diabetes Education Recognition Program is an IHS program that works towards high quality diabetes education programs by utilizing a three-staged accreditation scale. Native American programs in health care facilities can receive accreditation and guidance to effectively educate the community concerning diabetes self-management.[66]
Tribal Programs
Many tribes themselves have begun programs to address the diabetes epidemic, which can be specifically designed to address the concerns of the specific tribe. The Te-Moak Tribe of Western Shoshone have created their own diabetes program. With this program, they hope to promote healthly lifestyles with exercise and modified eating and behavior. The means of achieving these ends including "a Walking Club, 5 a Day Fruits and Vegetable, Nutrition teaching, Exercise focusing, 28 day to Diabetes Control, and Children's Cookbook."[67] Additionally, the Te-Moak tribe has constructed facilities to promote healthy lifestyles, such as a center to house the diabetes program and a park with a playground to promote active living.[67]
The Meskwaki Tribe of the Mississippi has also formed diabetes program to provide for the tribe's people. The Meskwaki Tribe facilitates their program in order to eliminate diabetes as a health concern through prevention and control of complications. The program has a team mentality, as community, education and clinical services are all involved as well as community organizations and members.[68]
There are many facets of this diabetes program, which include the distribution of diabetes information. This is achieved through bi-weekly articles in the Meskwaki Times educating the population about diabetes prevention and happenings in the program and additional educational materials available about diabetes topics. Other educational is spread through nutrition and diabetes classes, such as the Diabetes Prevention Intensive Lifestyle Curriculum Classes, and events like health fairs and walks. Medical care is also available. This includes bi-weekly diabetes clinics, screenings for diabetes and related health concerns and basic supplied.[68]
HIV-AIDS Programs

Multiple programs exist to address the HIV and AIDS concerns for Native Americans. Within the Indian Health Service, an HIV/AIDS Principal Consultant heads a vast HIV/AIDS Program. This program involves many different areas to address "treatment, prevention, policy, advocacy, monitoring, evaluation, and research."[69] They work through many social outputs to prevent the masses from the epidemic and enlist the help of many facilities to spread this message.[69]
The Indian Health Service also works with Minority AIDS Initiative to use funding to establish AIDS projects. Recently, this funding has been used to create testing, chronic care, and quality care initiatives as well as training and camps.[70] The Minority AIDS Initiative operates through the Ryan White HIV/AIDS Program, under the Public Health Service Act. This is in recognition of the disproportionate impact of HIV/AIDS on racial and ethnic minorities.[71]
There has also been a National Native HIV/AIDS Awareness Day held on March 20 for American Indians, Alaska Natives, and Native Hawaiians, with 2009 marking its third year. This day is held to:
- encourage Native people to get educated and to learn more about HIV/AIDS and its impact in their community;
- work together to encourage testing options and HIV counseling in Native communities; and
- help decrease the stigma associated with HIV/AIDS.[72]
This day takes place across the United States with many groups working in coordination, groups like the CDC and the National Native Capacity Building Assistance Network. By putting out press releases, displaying posters, and holding community events, these groups hope to raise awareness of the HIV/AIDS epidemic.[72]
Heart disease and stroke programs
The United States CDC contains a Division for Heart Disease and Stroke Prevention, and collects data and specifically releases information to form policy for Native Americans. They have identified many areas in which lifestyles of Native Americans need to be changed in order to greatly decrease the prevalence of heart disease and stroke.[62] One major concern to prevent is diabetes, which directly relates to the presence of heart disease. Many general health concerns also need to be addressed, according to the CDC's observations, including moderating alcohol use, eliminating tobacco use, maintaining health body weight, regularizing physical activity, diet, and nutrition, preventing and controlling high blood cholesterol, and preventing and controlling high blood pressure.[62]
The Indian Health Service works in collaboration with the University of Arizona College of Medicine to maintain the Native American Cardiology Program. This is a program that acknowledges the changes in lifestyle and economics in the recent past which have ultimately increased the prevalence of heart attacks, coronary disease, and cardiac deaths. The Native American Cardiology Program prides itself in its cultural understanding, which allows it to tailor health care for its patients.[73]
The program has many bases but has placed an emphasis on providing care to remote, rural areas in order for more people to be cared for. One of the more unique aspects of the Native American Cardiology Program is its telemedicine component. This branch also allows for health care to be made more accessible to Native Americans. This includes interpreting medical tests, offering specialist input and providing triage over the phone. The Native American Cardiology Program also has educational programs, such as lectures on cardiovascular disease and its impact, and outreach programs.[73]
See also
- Modern social statistics of Native Americans
- Indian Health Service
- New World Syndrome
- Alcohol and Native Americans
- Native American Health Center
General:
References
- ^ a b Francis, John M. (2005). Iberia and the Americas culture, politics, and history: A Multidisciplinary Encyclopedia. Santa Barbara, California: ABC-CLIO.
- ^ a b Marshall, Joseph (2005). The Journey of Crazy Horse, A Lakota History. Penguin Books.
- ^ Bruce Trigger. Natives and Newcomers: Canada’s “Heroic Age” Reconsidered. (Kingston: McGill-Queen’s University Press, 1985), 588-589.
- ^ a b c Waldman, Carl (2009). Atlas of the North American Indian. New York: Checkmark Books. p. 206.
- ^ Rossi, Ann. Two Cultures Meet: Native American and European. National Geographic Society. pp. 31–32. ISBN 0792286790.
- ^ Cowley, Geoffrey (1991). The Great Disease Migration. NewsWeek.
- ^ Robertson, R. G. (2001). Rotting Face Smallpox and the American Indian. New York: Caxton.
- ^ Watts, Sheldon (1999). Epidemics and History: Disease, Power and Imperialism. Yale University Press. ISBN 978-0-300-08087-2.
- ^ Lyon, William S. (1998). Encyclopedia of Native American Healing. W. W. Norton and Company.
- ^ Ramenofsky, Ann. 2003. Native American Disease History: Past, Present and Future Directions. World Archaeology. 35, no. 2: 241257.
- ^ a b c Ewald, Paul W. (2000). Plague Time: How Stealth Infections Cause Cancer, Heart Disease, and Other Deadly Ailments. New York: Free.
- ^ a b Dixon, David; Never Come to Peace Again: Pontiac's Uprising and the Fate of the British Empire in North America; (pg. 152-155); University of Oklahoma Press; 2005; ISBN 0-8061-3656-1
- ^ a b c d e Fenn, Elizabeth A. Biological Warfare in Eighteenth-Century North America: Beyond Jeffery Amherst; The Journal of American History, Vol. 86, No. 4, March, 2000
- ^ a b c Pontiac and the Indian Uprising; Peckham, Howard H.; University of Chicago Press; 1947; Pgs. 170, 226-7
- ^ Crucible of War: The Seven Years’ War and the Fate of Empire in British North America, 1754-1766; Anderson, Fred; New York: Knopf; 2000; Pgs. 541-2, 809n11; ISBN 0-375-40642-5
- ^ a b A Country Between: The Upper Ohio Valley and Its Peoples, 1724-1774; Michael N. McConnell; University of Nebraska Press; 1992; Pgs. 190-6
- ^ Empire of Fortune; Francis Jennings; W. W. Norton & Company; 1988; Pgs. 447-8
- ^ The Tainted Gift; Barbara Alice Mann; ABC-CLIO; 2009; Pgs. 1-18
- ^ The Conspiracy of Pontiac and the Indian War After the Conquest of Canada; Francis Parkman; Little, Brown & Company; Ninth Edition - 1898; Pgs. 38-42
- ^ Cherokee Medicine, Colonial Germs: An Indigenous Nation's Fight Against Smallpox, 1518–1824; Paul Kelton; University of Oklahoma Press; 2015; Pgs. 102-105
- ^ a b Biological and Toxin Weapons: Research, Development and Use from the Middle Ages to 1945; Mark Wheelis; Oxford University Press; 1999; Pgs. 17-26
- ^ Dowd, Gregory Evans (2004). War under Heaven: Pontiac, the Indian Nations, and the British Empire. New York: The Johns Hopkins University Press.
- ^ Philip Ranlet; "The British, the Indians, and smallpox: what actually happened at Fort Pitt in 1763?" Pennsylvania history (2000): 427-441. in JSTOR
- ^ Ecuyer, Simeon: Fort Pitt and letters from the frontier (1892)Captain Simeon Ecuyer's Journal: Entry of June 24,1763
- ^ Hanna, Charles A.:The wilderness trail : or, the ventures and adventures of the Pennsylvania traders on the Allegheny path, with some new annals of the old West, and the records of some strong men and some bad ones (1911) pg.366
- ^ Burke, James P., Pioneers of Second Fork (pgs. 19-22)
- ^ a b McCullough, John: The Captivity of John McCullough Personally written after eight years of captivity.
- ^ Ecuyer, Simeon: Fort Pitt and letters from the frontier (1892)Journal of Captain Simeon Ecuyer Entry June 2, 1763
- ^ Ecuyer, Simeon: Fort Pitt and letters from the frontier (1892)Journal of Captain Simeon Ecuyer: Entry of July 22, 1763
- ^ Ellis, F. and Hungerford, A.N.(Editors).History of that part of the Susquehanna and Juniata Valleysembraced in the counties of Mifflin, Juniata, Perry, Union and Snyder, in the commonwealth of Pennsylvania Published 1886 by Everts, Peck & Richards in Philadelphia.
- ^ McCullough, John: http://The Captivity of John McCullough Personally written after eight years of captivity.
- ^ Dixon, David, Never Come to Peace Again: Pontiac's Uprising and the Fate of the British Empire in North America (pg. 155)
- ^ Seaver James E.A Narrative of the Life of Mrs. Mary Jemison(1824)
- ^ a b "American Indian & Alaska Native (AI/AN) Populations". Office of Minority Health and Health Disparities, Centers for Disease Control and Prevention. November 30, 2010. Retrieved December 4, 2013.
- ^ Barnes, P.M., P.F. Adams, and E. Powell-Griner. (2010). Health Characteristics of the American Indian or Alaska Native Adult Population: United States, 2004-2008. Hyattsville, MD: U.S. Dept. of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics.
- ^ a b c d "American Indian/Alaska Native Profile – The Office of Minority Health." Home Page – The Office of Minority Health. 31 July 2009. Web. 01 Oct. 2009. <http://minorityhealth.hhs.gov/templates/browse.aspx?lvl=2&lvlID=52>
- ^ a b Young, T. Kue (1997). "Recent Health Trends in the Native Americans' Population". Population Research and Policy Review. 16: 147–67.
- ^ Deloria, Vine (1988). Custer Died For Your Sins, An Indian Manifesto. New York: University of Oklahoma Press. p. 55. ISBN 978-0-8061-2129-1.
- ^ Barnes, Patricia M. (2005). Vital and Health Statistics: Health Characteristics of the American Indian and Alaska Native Adult Population (356th ed.). Centers for Disease Control and Prevention.
- ^ a b 2005. Health Characteristics of the American Indian and Alaska Native Adult Population: U.S., 19992003 : Advance Data: From Vital and Health Statistics of the Centers for Disease Control and Prevention/National Center for Health Statistics;2005 ASI 41468.357;PHS 20051250, No. 356. n.p.:
- ^ "Division for Heart Disease and Stroke Prevention – AIAN Fact Sheet". Centers for Disease Control and Prevention. October 9, 2009.
- ^ (http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_aian.htm)
- ^ Duyff, Roberta Larson (2006). American Dietetic Association Complete Food and Nutrition Guide. New York: Wiley.
- ^ Bullock, Ann; Ronny A. Bell (2005). "Stress, trauma and coronary heart disease among Native Americans". American Journal of Public Health. 95: 2122-b-2123. doi:10.2105/AJPH.2005.072645.
- ^ a b "Cancer and American Indians/Alaska Natives". United States Department of Health and Human Services: Office of Minority Health. June 13, 2012. Retrieved September 7, 2012.
- ^ a b "Division of Diabetes Treatment and Prevention". Indian Health Service. Retrieved October 8, 2009.
- ^ a b c Narva, Andrew S. 2002. Kidney Disease in Native Americans. Journal of the National Medical Association. 94, no. 8: 738742.
- ^ a b c Joslin, Elliott P. (2005). Joslin's diabetes mellitus. Philadelphia: Lippincott Williams & Willkins.
- ^ Mogensen, Carl Erik (2000). The Kidney and Hypertension in Diabetes Mellitus. New York: Springer.
- ^ a b c d Ekoé, Jean-Marie; Zimmet, Paul; Williams, Rhys, eds. (2001). The Epidemiology of Diabetes Mellitus: An International Perspective. New York: Wiley.
- ^ Centers for Disease Control and Prevention (CDC) (2013-02-27), OUR CULTURES ARE OUR SOURCE OF HEALTH, retrieved 2016-05-06
- ^ a b c "Mental Health - The Office of Minority Health". minorityhealth.hhs.gov. Retrieved 2016-05-05.
- ^ a b kpolisse (2016-04-25). "New IHS Head Focused on Quality, Accountability". Indian Country Today Media Network.com. Retrieved 2016-05-05.
- ^ Hebblethwaite, Cordelia. 2014. #BBCtrending: Native Americans reject 'super drunk' label. BBC [News]
- ^ Sandefur, Gary D (1996). Changing numbers, Changing needs: American Indian demography and public health. National Academy Press. ISBN 978-0-309-17529-6.
- ^ Crawford, Michael H. (2001). The Origins of Native Americans Evidence from Anthropological Genetics. New York: Cambridge University Press.
- ^ Fan, Hung (2004). AIDS Science and Society, Fourth Edition. Jones and Bartlett Series in Biology. New York: Jones and Bartlett.
- ^ a b Izadi, Elahe. 2016. Your Assumptions About Native Americans and Alcohol Are Wrong. Washington Post – Blogs. .
- ^ a b "The Indian Health Service Fact Sheets". Retrieved October 11, 2009.
- ^ a b "HIV/AIDS among American Indians and Alaska Natives — Factsheets". Centers for Disease Control and Prevention. Retrieved October 6, 2009.
- ^ "Stroke and American Indians/Alaska Natives". Office of Minority Health. Retrieved October 11, 2009.
- ^ a b c "Division for Heart Disease and Stroke Prevention – AIAN Fact Sheet". Centers for Disease Control and Prevention. Retrieved October 11, 2009.
- ^ "Introduction to IHS by Dr Yvette Roubideaux". Indian Health Service. Retrieved October 9, 2009.
- ^ a b c "National Diabetes Wellness Program". Centers for Disease Control and Prevention. Retrieved October 9, 2009.
- ^ "Eagle Books | Native Diabetes Wellness Program". www.cdc.gov. Retrieved 2016-05-06.
- ^ a b c d e f g "Division of Diabetes Treatment and Prevention". Indian Health Service. Retrieved October 9, 2009.
- ^ a b "Special Diabetes Program". Te-Moak Tribe of Western Shoshone. Retrieved October 13, 2009.
- ^ a b "Sac & Fox Tribe – Diabetes & Wellness Program". Official Site of the Meskwaki Nation. Retrieved October 13, 2009.
- ^ a b "IHS HIV/AIDS Program". Indian Health Service. Retrieved October 11, 2009.
- ^ "IHS HIV/AIDS Program Minority AIDS Initiative". Indian Health Service. Retrieved October 11, 2009.
- ^ "HRSA – Part F Minority AIDS Initiative". Health Resources and Services Administration. Retrieved October 11, 2009.
- ^ a b "2009 National Native HIV/AIDS Awareness Day". National Native American AIDS Prevention Center. Retrieved October 11, 2009.
- ^ a b "Native American Cardiology Program at UMC". University Medical Center Tucson, Arizona. Retrieved October 14, 2009.