
Talk:Tianeptine: Difference between revisions
→How does it work?: possible explanation for anti depressive function |
|||
| Line 81: | Line 81: | ||
::there's zero evidence even to support that this has anything to do with tianeptine. for all we know they injected motor oil into their veins. it's important to note that the video mentioned is very graphic, quite disgusting, and not for the faint of heart. for that matter, i've removed the link to the video, since it has no demonstrated connection to this article. there's no point in spreading misinformation, based on a shock-website that claims something. if a russian speaker provides an actual translation, fine, then maybe it's worth further review. until then, just as the site name suggests, it's 'totally crap'. [[User:Anastrophe|Anastrophe]] ([[User talk:Anastrophe|talk]]) 18:02, 31 May 2009 (UTC) |
::there's zero evidence even to support that this has anything to do with tianeptine. for all we know they injected motor oil into their veins. it's important to note that the video mentioned is very graphic, quite disgusting, and not for the faint of heart. for that matter, i've removed the link to the video, since it has no demonstrated connection to this article. there's no point in spreading misinformation, based on a shock-website that claims something. if a russian speaker provides an actual translation, fine, then maybe it's worth further review. until then, just as the site name suggests, it's 'totally crap'. [[User:Anastrophe|Anastrophe]] ([[User talk:Anastrophe|talk]]) 18:02, 31 May 2009 (UTC) |
||
:::And, of course, it somehow (in some fucked up fantasy world of yours) matters what website it is hosted on when it's obvious that physicians are treating the patients in the video. If what the doctors are saying backs up claims that Tianeptine was the culprit, why should it be dismissed? Just because you don't feel like asking for someone to translate it doesn't mean you should be an asshole and claim it's bogus. Do you speak Russian? Are you a physician? Then how the hell would you know? It's self-righteous assholes like you that are ruining wikipedia. [[Special:Contributions/66.153.217.152|66.153.217.152]] ([[User talk:66.153.217.152|talk]]) 08:11, 11 June 2009 (UTC) |
:::And, of course, it somehow (in some fucked up fantasy world of yours) matters what website it is hosted on when it's obvious that physicians are treating the patients in the video. If what the doctors are saying backs up claims that Tianeptine was the culprit, why should it be dismissed? Just because you don't feel like asking for someone to translate it doesn't mean you should be an asshole and claim it's bogus. Do you speak Russian? Are you a physician? Then how the hell would you know? It's self-righteous assholes like you that are ruining wikipedia. [[Special:Contributions/66.153.217.152|66.153.217.152]] ([[User talk:66.153.217.152|talk]]) 08:11, 11 June 2009 (UTC) |
||
::::O yeah... that tirade helped prove your point. [[Special:Contributions/71.86.152.127|71.86.152.127]] ([[User talk:71.86.152.127|talk]]) 17:38, 27 September 2009 (UTC) |
|||
Revision as of 17:38, 27 September 2009
| This is the talk page for discussing improvements to the Tianeptine article. This is not a forum for general discussion of the article's subject. |
Article policies
|
| Find sources: Google (books · news · scholar · free images · WP refs) · FENS · JSTOR · TWL |
| Pharmacology B‑class High‑importance | ||||||||||
| ||||||||||

tianeptine has never undergone the gold standard i.e. testing against a tricyclic antidepressant compared against placebo. Why not,I do not know. I cannot believe that it has not been done as the first publication about tianeptine date from 1989 This site seems very close to the talk of pharmaceutic representative of Ardix. One should ask why this fantastic substance has not been approved by the FDA.
- Um, because the patent that Servier has on tianeptine has expired? Fortunately, Vela Pharmaceuticals (acquired recently by Pharmos) is interested. Yes, I know it's an...interesting website, but they're the only ones who've explained why Sevier hasn't tried marketing it in the US, besides the fact that so many people here have grown up on the idea that depression is merely a serotonin defiency. This is probably why Pharmos is marketing it for irritable bowel syndrome.--Rmky87 21:08, 8 July 2006 (UTC)
A strong antidepressant?
Unlike neuroleptics or anxiolytics/(minor) tranquilizers, antidepressants effectivity can't be quantified by any way. An antidepressant either works in a depressive patient, or it does partially or not at all. There were and are some approaches to qualify particular drug for particular conditions of depressive disorder (e.g. classical tricyclics, such as imipramine, amitriptyline or clomipramine for severe major depression, or maprotiline for somatised ("larved depression" by Kielholz) depression, or SSRI's for anxiety- and/or OCD-accompagnied depression or high-dosed venlafaxine for torpid adynamic depressive disorders etc.), but in fact, none of these are much reliable. If you say "strong neuroleptic/antipsychotic", I would most likely imagine either a neuroleptic of high neuroleptic potency/with high chlorpromazine index, such as haloperidol, benperidol or fluphenazine, or a neuroleptic/antipsychotic, that works in psychotic patient that is refractory to many other drugs (such as clozapine). If I read "strong tranquilizer", I associate a potent benzodiazepine, like lorazepam, clonazepam or alprazolam.
But what is a "strong antidepressant"? The one that needs low relative doses (in mg/day)? Than, probably reboxetine and (S)-citalopram would be the most potent (doses of 4-12 mg/day and 5-20mg/day, respectivelly). Or the one that works for patients that are refractory to others and there is a statistically relative occurence of such algorithm, as in case of clozapine in antipsychotic-refractory schizophrenic psychoses? None of these criteria fits for tianeptine, and they are not relevant. Tianeptine is, according to the prescribing information of the manufacturer, suitable for treatment of medium-severe depressions without psychotic features, in somatic and anxiety comorbidities, and in the treatment of alcoholics or illcit drug dependant patients. I don't see any reason to mark the antidepressant effects of tianeptine as "strong", or, vice versa, why not to mark antidepressive effects of e.g. amitriptyline, clomipramine, dibenzepine, sertraline, mirtazapine or venlafaxine as "strong".
As I wrote, the only thing that makes an antidepressant "strong/potent" is the extent, in which it alleviates the symptoms of depressive disorder in every single patient, and thus is necessarily highly individual.--Spiperon 21:36, 15 October 2006 (UTC)
- I partially agree. The use of the term "strong" is not supported, as it is too vague. In my experience, people colloquially take this to mean "unselective" or "lots of side-effects".
- However, there are objective metrics to the efficacy of an antidepressant medication. For instance, tranylcypromine achieves remission in 85% of treatment refractory (i.e. failed to respond to 3 prior drugs in trials of adequate dose and duration), and is comparable to ECT. Imipramine is also quite effective, although the side-effects are often intolerable. If you could deliver 60mg cocaine over a 24 hour period with a slow-release capsule or a patch, along with something to counter its toxicity, you'd probably see even better stats, although that strays into the territory of definite abuse potential.
- The question is really how likely the drug is to be effective in a randomly selected patient in clinical practice, given adequate doses over an adequate period of time, as well as how long this improvement is likely to last.
- However, that question is only rarely answered, as drug trials have strict inclusion and exclusion criterion (more than one specialist has commented that you never encounter these patients in a clinical setting), and usually have a limited duration (typically 6 months or less). Basically, the question is actively sidestepped by the manufacturers. This makes financial sense, much in the same way as not actively comparing with antidepressants that are viable and on-patent. TCAs are preferred, with at least one source citing imipramine as the "gold standard". Many still use only inactive placebo or only TCAs, making the dataset harder to verify for inclusion in a meta-analysis.
- The availability of secondary sources on this aspect is thus generally limited to older drugs, such as the unselective MAOIs and the TCAs, most of which have been thoroughly studied.
- Therapeutic interval is not a good metric, as you pointed out, both due to the difference in Ki values (e.g. NE Ki >10000nM/L for reboxetine vs apx 4000nM/L for methamphetamine), absorption, half-life, etc. and such things as the balance between increased tonus and increased phasic transmission.
- In short, the word "strong" should not be used to describe any antidepressant. "Potent" could possibly be used in the sense that it is used with other drugs (degree of activity at the given receptors). All in all, however, there is a good argument that tianeptine can be a more effective drug than many others on the market, based on good efficacy at the recommended dose and an apparently large therapeutic index.
- Zuiram 05:20, 25 February 2007 (UTC)
How does it work?
Can someone address the obvious contradiction? 68.0.113.54 05:17, 30 January 2007 (UTC)
- And what would that be?--Rmky87 21:33, 30 January 2007 (UTC)
- (S)he is probably referring to the serotonin hypothesis, and the apparent contradiction between the SSRIs showing antidepressant efficacy and tianeptine showing the same, despite the opposite mode of action.
- The party line is that the increased reuptake of 5HT from the synapse causes a buildup of 5HT in the vesicles. This would be a somewhat plausible explanation if the effect were similar to the SSRIs, as a significant amount of 5HT is destroyed by MAO-A in the synapse under usual circumstances. With faster reuptake, you would see less 5HT destroyed, and consequently a similar increase in stored 5HT as is seen with MAO-inhibitors.
- This theory is not as simple as it seems, however. SSRIs appear to owe their antidepressant efficacy to an upregulation of the postsynaptic D2-receptors in downstream systems, along with a downregulation of central beta-receptors. The former has a mood-brightening effect, while the latter has the effect of lessening the impact of emotional context in stored memories. Also, there may be some lessening of emotional lability due to downregulation of non-D2 dopamine-receptors; this would explain the potential for akathisia, through the same mechanism as the neuroleptics (reducted transmission at D4 receptors, if memory serves).
- Tianeptine would presumably give a moderate, but fairly rapid, increase in tonic and phasic dopaminergic activity (accounting for the high-dose abuse potential) due to disinhibition, followed by a longer term increase in vesicular storage of 5HT with a subsequent increase in phasic 5HT activity without the tonic increase seen with SSRIs and MAOIs. Again, it's been a while since I researched tianeptine, so my memory may not be an accurate guide here.
- There is no contradiction, though.
- Zuiram 05:33, 25 February 2007 (UTC)
- Could you (or someone else) write a bit about this in the article? --137.205.76.219 16:53, 17 March 2007 (UTC)
- I agree that an expansion (if only theoretical) would be helpful as little other action information appears on web searches. Also given the drugs use in erectile dysfunction could comment be made on its action in this regard cf SSRIs?
- I went through Serotonin withdrawal (so called Serotonin syndrome) because of being withdrawn from Clomipramine too quickly. The effects were a bit extreme and not altogether unpleasant. I asked the doctor and did my own research and the explanation was a lowered number of receptors for serotonin in the brain from the bodies natural tendency to be adaptive to the bioavailable levels. I started wishing for a drug with a short duration that reduced available serotonin in order to instigate small periods of Serotonin syndrome and thus eventually force the brain to increase the number of receptors beyond it's trained baseline. Tianeptine is short lived and lowers serotonin levels. Could it be forcing the receptor levels up?
- The euphoria described by patients is easy to believe; my experiences with serotonin withdrawal left me energized and extremely horny. I saw somewhere that being in love men's brain chemistry increases to induce cuddling (oxytosin/serotonin increases - I can't remember) and in women there was serotonin decreases to encourage them to higher sex drives. Just some thoughts and WK:OR so these thoughts would need to be sourced. (done anonymously on purpose) 71.86.156.73 (talk) 12:45, 9 August 2009 (UTC)
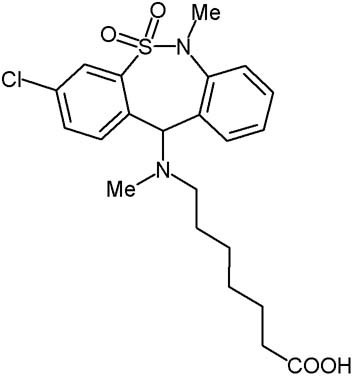
The molecular image is still wrong.
Is someone going to fix this at some point? The conspicuous lack of chlorine anywhere in the image should have clued in anyone who actually looks at it.
When someone finally does attempt to fix it, please note:
http://www.biopsychiatry.com/tianeptine/tianeptine.jpg
{kind=link}
This image is also wrong. Count the carbons.
http://www.genome.jp/dbget-bin/www_bget?dr+D02575
This image is correct.
--76.209.58.121 14:34, 27 February 2007 (UTC)
- Fixed, thank you for noticing. Fvasconcellos 16:56, 27 February 2007 (UTC)
Irritable Bowel Syndrome/US Approval Process
Vera pharmaceuticals obtained a patent on the drug in the U.S. (for irritable bowel syndrome) and is going through the approval process to try to pass it through the FDA.
History of Tianeptine: Rejection in America
Anyone skilled/knowledgeable enough to search and document how and why Tianeptine hasn't been submited/approved in USA/Canada ? Marty (whereismarty@hotmail.com) 69.70.202.20 (talk) 20:39, 2 June 2008 (UTC)
Abuse
Moved the part about abuse in Russia into the abuse section. Also, there's no hits for "tianeptine abuse" (or even "tianeptine") on Google News, so I added a citation needed tag. Apophenic (talk) 20:43, 30 October 2008 (UTC)
- There's a video going around showing the potential side effects of intravenous tianeptine injection.
- No way to know what that is without speaking Russian, of course. One of the subjects makes a motion as if to say he injected the tianeptine into his hand, between the fingers. The effects of whatever they injected are quite shocking. Skin dissolved right to the bone...
- 24.68.36.117 (talk) 07:28, 31 May 2009 (UTC)
- there's zero evidence even to support that this has anything to do with tianeptine. for all we know they injected motor oil into their veins. it's important to note that the video mentioned is very graphic, quite disgusting, and not for the faint of heart. for that matter, i've removed the link to the video, since it has no demonstrated connection to this article. there's no point in spreading misinformation, based on a shock-website that claims something. if a russian speaker provides an actual translation, fine, then maybe it's worth further review. until then, just as the site name suggests, it's 'totally crap'. Anastrophe (talk) 18:02, 31 May 2009 (UTC)
- And, of course, it somehow (in some fucked up fantasy world of yours) matters what website it is hosted on when it's obvious that physicians are treating the patients in the video. If what the doctors are saying backs up claims that Tianeptine was the culprit, why should it be dismissed? Just because you don't feel like asking for someone to translate it doesn't mean you should be an asshole and claim it's bogus. Do you speak Russian? Are you a physician? Then how the hell would you know? It's self-righteous assholes like you that are ruining wikipedia. 66.153.217.152 (talk) 08:11, 11 June 2009 (UTC)
- O yeah... that tirade helped prove your point. 71.86.152.127 (talk) 17:38, 27 September 2009 (UTC)
- And, of course, it somehow (in some fucked up fantasy world of yours) matters what website it is hosted on when it's obvious that physicians are treating the patients in the video. If what the doctors are saying backs up claims that Tianeptine was the culprit, why should it be dismissed? Just because you don't feel like asking for someone to translate it doesn't mean you should be an asshole and claim it's bogus. Do you speak Russian? Are you a physician? Then how the hell would you know? It's self-righteous assholes like you that are ruining wikipedia. 66.153.217.152 (talk) 08:11, 11 June 2009 (UTC)
- there's zero evidence even to support that this has anything to do with tianeptine. for all we know they injected motor oil into their veins. it's important to note that the video mentioned is very graphic, quite disgusting, and not for the faint of heart. for that matter, i've removed the link to the video, since it has no demonstrated connection to this article. there's no point in spreading misinformation, based on a shock-website that claims something. if a russian speaker provides an actual translation, fine, then maybe it's worth further review. until then, just as the site name suggests, it's 'totally crap'. Anastrophe (talk) 18:02, 31 May 2009 (UTC)