
Eustachian tube
| Eustachian Tube | |
|---|---|
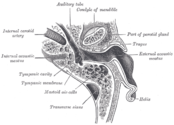
 Middle ear, with auditory tube at bottom right. | |
| Details | |
| Precursor | first branchial pouch |
| Identifiers | |
| Latin | Tuba auditiva, tuba auditivea, tuba auditoria |
| MeSH | D005064 |
| TA98 | A15.3.02.073 |
| TA2 | 6926 |
| FMA | 9705 |
| Anatomical terminology | |
The Eustachian tube /juːˌsteɪ.ʃənˈtjuːb/, also known as the auditory tube or pharyngotympanic tube,[1] is a tube that links the nasopharynx to the middle ear. It is a part of the middle ear. In adult humans the Eustachian tube is approximately 35 mm (1.4 in) long and 3 mm (0.12 in) in diameter. [2] It is named after the sixteenth-century anatomist Bartolomeo Eustachi.[3]
In humans and other land animals the middle ear (like the ear canal) is normally filled with air. Unlike the open ear canal, however, the air of the middle ear is not in direct contact with the atmosphere outside the body. The Eustachian tube connects from the chamber of the middle ear to the back of the nasopharynx.
Normally, the Eustachian tube is collapsed, but it gapes open both with swallowing and with positive pressure. When taking off in an airplane, the surrounding air pressure goes from higher (on the ground) to lower (in the sky). The air in the middle ear expands as the plane gains altitude, and pushes its way into the back of the nose and mouth. On the way down, the volume of air in the middle ear shrinks, and a slight vacuum is produced. Active opening of the Eustachian tube is required to equalize the pressure between the middle ear and the surrounding atmosphere as the plane descends. The diver also experiences this change in pressure, but with greater rates of pressure change; active opening of the Eustachian tube is required more frequently as the diver goes deeper into higher pressure.
Structure

The Eustachian tube extends from the anterior wall of the middle ear to the lateral wall of the nasopharynx, approximately at the level of the inferior nasal concha. It consists of a bony part and a cartilaginous part.
A portion of the tube (1/3) proximal to the middle ear is made of bone; this bony part is about 12 mm in length. It begins in the carotid wall of the tympanic cavity, below the septum canalis musculotubarii, and, gradually narrowing, ends at the angle of junction of the squama and the petrous portion of the temporal bone, its extremity presenting a jagged margin which serves for the attachment of the cartilaginous portion of the rest of the tube,[4] and this raises a tubal elevation, the torus tubarius, in the nasopharynx where it opens.
There are four muscles associated with the function of the Eustachian tube:
- Levator veli palatini (innervated by the vagus nerve)
- Salpingopharyngeus (innervated by the vagus nerve)
- Tensor tympani (innervated by the mandibular nerve of CN V)
- Tensor veli palatini (innervated by the mandibular nerve of CN V)
Cartilaginous part
The cartilage of pharyngotympanic tube, about 24 mm. in length, is formed of a triangular plate of elastic fibrocartilage, the apex of which is attached to the margin of the medial end of the osseous portion of the tube, while its base lies directly under the mucous membrane of the nasal part of the pharynx, where it forms an elevation, the torus tubarius or cushion, behind the pharyngeal orifice of the tube.
The upper edge of the cartilage is curled upon itself, being bent laterally so as to present on transverse section the appearance of a hook; a groove or furrow is thus produced, which is open below and laterally, and this part of the canal is completed by fibrous membrane. The cartilage lies in a groove between the petrous part of the temporal bone and the great wing of the sphenoid; this groove ends opposite the middle of the medial pterygoid plate. The cartilaginous and bony portions of the tube are not in the same plane, the former inclining downward a little more than the latter. The diameter of the tube is not uniform throughout, being greatest at the pharyngeal orifice, least at the junction of the bony and cartilaginous portions, and again increased toward the tympanic cavity; the narrowest part of the tube is termed the isthmus.
The position and relations of the pharyngeal orifice are described with the nasal part of the pharynx. The mucous membrane of the tube is continuous in front with that of the nasal part of the pharynx, and behind with that of the tympanic cavity; it is covered with ciliated pseudostratified columnar epithelia and is thin in the osseous portion, while in the cartilaginous portion it contains many mucous glands and near the pharyngeal orifice a considerable amount of adenoid tissue, which has been named by Gerlach the tube tonsil.
The tube is opened during swallowing by contraction of the tensor veli palatini and levator veli palatini, muscles of the soft palate.[1]
Development
The Eustachian tube is derived from the ventral part of the first pharyngeal pouch and second endodermal pouch, which during embryogenesis forms the tubotympanic recess. The distal part of the tubotympanic sulcus gives rise to the tympanic cavity, while the proximal tubular structure becomes the Eustachian tube. It helps transformation of sound waves.
Function
Pressure equalization
Under normal circumstances, the human Eustachian tube is closed, but it can open to let a small amount of air through to prevent damage by equalizing pressure between the middle ear and the atmosphere. Pressure differences cause temporary conductive hearing loss by decreased motion of the tympanic membrane and ossicles of the ear.[5] Various methods of ear clearing such as yawning, swallowing, or chewing gum, may be used intentionally to open the tube and equalize pressures. When this happens, humans hear a small popping sound, an event familiar to aircraft passengers, scuba divers, or drivers in mountainous regions. Devices assisting in pressure equalization include an ad hoc balloon applied to the nose, creating inflation by positive air pressure.[6] Some people learn to voluntarily 'click' their ears, together or separately, performing a pressure equalizing routine by opening their Eustachian tubes when pressure changes are experienced, as in ascending/descending in aircraft, mountain driving, elevator lift/drops, etc. Some are even able to deliberately keep their Eustachian tubes open for a brief period, and even increase or decrease air pressure in the middle ear. The 'clicking' can actually be heard audibly by putting one's ear to another's while performing the clicking sound. This voluntary control may be first discovered when yawning or swallowing, or by other means (above). Those who develop this ability may discover that it can be done deliberately without force even when there are no pressure issues involved.
Mucus drainage
The Eustachian tube also drains mucus from the middle ear. Upper respiratory tract infections or allergies can cause the Eustachian tube, or the membranes surrounding its opening to become swollen, trapping fluid, which serves as a growth medium for bacteria, causing ear infections. This swelling can be reduced through the use of decongestants such as pseudoephedrine, oxymetazoline, and phenylephrine.[7] Ear infections are more common in children because the tube is horizontal and shorter, making bacterial entry easier, and it also has a smaller diameter, making the movement of fluid more difficult. In addition, children's developing immune systems and poor hygiene habits make them more prone to upper respiratory infections.
Clinical significance
Otitis media, or inflammation of the middle ear, commonly affects the Eustachian tube. Children under 7 are more susceptible to this condition, one theory being that this is because the Eustachian tube is shorter and at more of a horizontal angle than in the adult ear. Others argue that susceptibility in this age group is related to immunological factors and not Eustachian tube anatomy.[citation needed]
Barotitis, a form of barotrauma, may occur when there is a substantial difference in air or water pressure between the outer and the inner ear — for example, during a rapid ascent while scuba diving, or during sudden decompression of an aircraft at high altitude.
Some people are born with a dysfunctional Eustachian tube[8] that is much slimmer than usual. The cause may be genetic, but it has also been posited as a condition in which the patient did not fully recover from the effects of pressure on the middle ear during birth (retained birth compression).[9][unreliable medical source] It is suggested that Eustachian tube dysfunction can result in a large amount of mucus accumulating in the middle ear, often impairing hearing to a degree. This condition is known as otitis media with effusion, and may result in the mucus becoming very thick and glue-like, a condition known as glue ear.
A patulous Eustachian tube is a rare condition in which the Eustachian tube remains intermittently open, causing an echoing sound of the person's own heartbeat, breathing, and speech. This may be temporarily relieved by holding the head upside down.
Smoking can also cause damage to the cilia that protect the Eustachian tube from mucus, which can result in the clogging of the tube and a buildup of bacteria in the ear, leading to a middle ear infection.[10]
Recurring and chronic cases of sinus infection can result in Eustachian tube dysfunction caused by excessive mucus production which, in turn, causes obstruction to the openings of the Eustachian tubes.
Surgical Eardrum Piercing
In severe cases of childhood inner ear infections and Eustachion tube blockage, ventilation can be provided by a surgical puncturing of the eardrum to permit air equalization, known as Myringotomy. The eardrum would normally naturally heal and close the hole, so a tiny plastic rimmed grommet is inserted into the hole to hold it open. This is known as a Tympanostomy tube. As a child grows, the tube is eventually naturally expelled by the body. Longer-lasting vent grommets with larger flanges have been researched, but these can lead to permanent perforation of the eardrum.
Permanent venting to external ear canal
Surgical implantation of permanent bypasses around the eardrum have also been studied, though these suffer from blockage issues, requiring frequent manual cleaning. These also can lead to inner ear infection due to the direct path from the external to the internal ear.[11]
Eustachian tube prosthesis
Another approach to permitting inner ear drainage is the use of a prosthesis inserted into the Eustachian tube, to assist in holding the tube open. The prosthesis does not necessarily hold the tube completely open all the time, but may instead lightly brace the tissue walls of a narrow tube to assist in venting.
One such example invented in 1978 is a silicone tube with a flange at the top, which keeps it from dislodging and sliding out into the throat.[12] However, in a study in 1978 it was not found to be effective for long-term use, and would eventually become internally blocked with mucous or otitis media, or dislodged from its position.[13]
Removal of excessive tube tissue
Debridement has also been studied as a solution to inability to open the Eustachian tube. Hypertrophy (excessive growth) of the cells that produce mucus can make the tube hard to open, and the procedure to reduce the growth is known as "microdebrider eustachian tuboplasty".[14]
Other animals
In the equids (horses) and some rodent-like species such as the desert hyrax, an evagination of the eustachian tube is known as the guttural pouch and is divided into medial and lateral compartments by the stylohyoid bone of the hyoid apparatus. This is of great importance in equine medicine as the pouches are prone to infections, and, due to their intimate relationship to the cranial nerves (VII, IX, X, XI) and the internal and external carotid artery, various syndromes may arise relating to which is damaged. Epistaxis (nosebleed) is a very common presentation to veterinary surgeons and this may often be fatal unless a balloon catheter can be placed in time to suppress bleeding.
Additional images
-
 External and middle ear, opened from the front; right side.
External and middle ear, opened from the front; right side. -
 Horizontal section through left ear; upper half of section
Horizontal section through left ear; upper half of section -
 View of the inner wall of the tympanum (enlarged)
View of the inner wall of the tympanum (enlarged) -
 The right membrana tympani with the hammer and the chorda tympani, viewed from within, from behind, and from above
The right membrana tympani with the hammer and the chorda tympani, viewed from within, from behind, and from above




See also
References
- ^ a b Keith L. Moore; Arthur F. Dalley; A. M. R. Agur (13 February 2013). Clinically Oriented Anatomy. Lippincott Williams & Wilkins. p. 970. ISBN 978-1-4511-1945-9.
- ^ http://www.medicinenet.com/eustachian_tube_problems/article.htm
- ^ Eustachian tube at Who Named It?
- ^ 'Ear - Dissector Answers at University of Michigan Medical School
- ^ Page 152 in:Rex S. Haberman (2004). Middle Ear and Mastoid Surgery. New York: Thieme Medical Pub. ISBN 1-58890-173-4.
- ^ Leunig, A.; Mees, K. (2008). "Mittelohrbelüftung mit dem Otovent®-Latexmembran- System". Laryngo-Rhino-Otologie. 74 (6): 352–354. doi:10.1055/s-2007-997756. PMID 7662078.
- ^ "Middle Ear, Eustachian Tube, Inflammation/Infection Treatment & Management". Medscape. Retrieved 2014-08-06.
- ^ Eustachian Tube Function and Dysfunction at Baylor College of Medicine
- ^ "FAQs - Cranial Osteopathy". The Children's Clinic. Archived from the original on 2010-05-29. Retrieved 2008-12-23.
- ^ Dubin MG, Pollock HW, Ebert CS, Berg E, Buenting JE, Prazma JP (2002). "Eustachian tube dysfunction after tobacco smoke exposure". Otolaryngology - Head and Neck Surgery. 126 (1): 14–19. doi:10.1067/mhn.2002.121320. PMID 11821759.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ US Patent #3,982,545, "Middle ear aeration and implant", issued Aug 22, 1974 http://www.google.com/patents/US3982545 Accessed Feb 4, 2016
- ^ US Patent #4015607, "Eustachian tube prosthesis", issued Jan 23, 1976 http://www.google.com/patents/US4015607 Accessed Feb 4, 2016
- ^ J.W. Wright III et al. “The Eustachian tube prosthesis revisited”, Journal of Oto-Rhino-Laryngology, vol. 86, 1978, pp. 834-837
- ^ Microdebrider eustachian tuboplasty: A preliminary report. Otolaryngol Head Neck Surg. 2007 Mar;136(3):422-7. http://www.ncbi.nlm.nih.gov/pubmed/17321871