
Gallbladder cancer
| Gallbladder cancer | |
|---|---|
 | |
| Specialty | Gastroenterology Hepatology Oncology |
| Symptoms | Abdominal pain, Bloating, Fever, Unexplained weight loss, Nausea, Yellowing of the skin, although some people may have no symptoms[1] |
| Complications | Cancer spreading to other parts of the body |
| Usual onset | Above 65 years old[2] |
| Types | Adenocarcinoma (most common), Squamous cell carcinoma (more rare)[3] |
| Causes | Unknown[1] |
| Risk factors | History of Gallstones and other Gallbladder diseases |
| Diagnostic method | Blood tests, medical imaging, examination of the Bile duct |
| Differential diagnosis | Other types of cancer in the Digestive system |
| Treatment | Surgery, Radiation therapy, Chemotherapy[4] |
| Prognosis | Five-year survival rate ~19% (USA) (January, 2020)[5] |
| Frequency | ~3,700 cases per year (USA)[6] |
| Deaths | ~2,000 deaths per year (USA)[6] |
Gallbladder cancer is a relatively uncommon cancer, with an incidence of fewer than 2 cases per 100,000 people per year in the United States.[7] It is particularly common in central and South America, central and eastern Europe, Japan and northern India; it is also common in certain ethnic groups e.g. Native American Indians and Hispanics.[8] If it is diagnosed early enough, it can be cured by removing the gallbladder, part of the liver and associated lymph nodes. Most often it is found after symptoms such as abdominal pain, jaundice and vomiting occur, and it has spread to other organs such as the liver.
It is a rare cancer that is thought to be related to gallstones building up, which also can lead to calcification of the gallbladder, a condition known as porcelain gallbladder. Porcelain gallbladder is also rare. Some studies indicate that people with porcelain gallbladder have a high risk of developing gallbladder cancer, but other studies question this. The outlook is poor for recovery if the cancer is found after symptoms have started to occur, with a 5-year survival rate of close to 3%.[citation needed]
Signs and symptoms
[edit]- Steady pain in the upper right abdomen
- Indigestion (dyspepsia)
- Bilious vomit
- Weakness
- Loss of appetite
- Weight loss
- Jaundice and vomiting due to obstruction
Early symptoms mimic gallbladder inflammation due to gallstones. Later, the symptoms may be that of biliary and stomach obstruction.[citation needed]
Of note, Courvoisier's law states that in the presence of a palpably enlarged gallbladder which is nontender and accompanied with mild painless jaundice, the cause is unlikely to be gallstones. This implicates possible malignancy of the gallbladder or pancreas, and the swelling is unlikely due to gallstones due to the chronic inflammation associated with gallstones leading to a shrunken, non-distensible gallbladder. However, the original observations of Ludwig Georg Courvoisier, published in Germany in 1890, were not originally cited as a law, and no mention of malignancy or pain (tenderness) was made. These points are commonly misquoted or confused in the medical literature.[9]
Risk factors
[edit]- Gender— approximately twice as common in women than men, usually in seventh and eighth decades
- Obesity
- Chronic cholecystitis and cholelithiasis
- Primary sclerosing cholangitis[10]
- Chronic typhoid infection of gallbladder; chronic Salmonella typhi carriers have 3 to 200 times higher risk of gallbladder cancer than non-carriers and 1–6% lifetime risk of development of cancer[11]
- Various single nucleotide polymorphisms (SNPs) have been shown to be associated with gallbladder cancer; however, existing genetic studies in GBC susceptibility have so far been insufficient to confirm any association[12]
- Gallbladder polyps[13]
- Calcified gallbladder wall (porcelain gallbladder)[13]
- Congenital abnormalities of the bile duct such as choledochal cyst[13]
Diagnosis
[edit]Early diagnosis is not generally possible. People at high risk, such as women or Native Americans with gallstones, are evaluated closely. Transabdominal ultrasound, CT scan, endoscopic ultrasound, MRI, and MR cholangio-pancreatography (MRCP) can be used for diagnosis. A large number of gallbladder cancers are found incidentally in patients being evaluated for cholelithiasis, or gallstone formation, which is far more common.[14] A biopsy is the only certain way to tell whether or not the tumorous growth is malignant.[15]
-
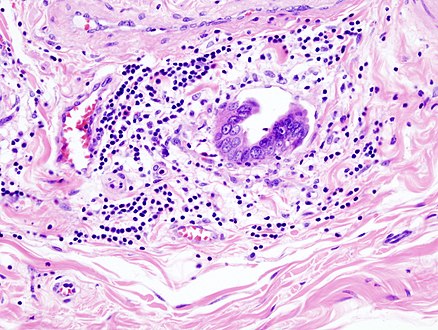 Gallbladder adenocarcinoma lymphatic invasion histopathology
Gallbladder adenocarcinoma lymphatic invasion histopathology -
 Incidentally discovered gallbladder cancer (adenocarcinoma) following a cholecystectomy.
Incidentally discovered gallbladder cancer (adenocarcinoma) following a cholecystectomy. -
 Gallbladder adenocarcinoma histopathology
Gallbladder adenocarcinoma histopathology
_lymphatic_invasion_histopathology.jpg)
_histopathology.jpg)
_histopathology.jpg)
Differential diagnosis
[edit]Xanthogranulomatous cholecystitis (XGC) is a rare form of gallbladder disease which mimics gallbladder cancer although it is not cancerous.[16][17] It was first discovered and reported in the medical literature in 1976 by J.J. McCoy Jr., and colleagues.[16][18]
Treatment
[edit]If detected early in a stage where it has not spread, gallbladder cancer can be treated by surgery. Surgery for gallbladder cancer is called radical cholecystectomy or extended cholecystectomy.[19] It entails the removal of gallbladder along with adequate removal of its liver bed to the healthy tissue. The lymph nodes in the vicinity are also removed. Sometimes removal of a large part of the liver called hepatectomy is required to completely remove the tumor. The bile duct if involved also needs to be removed.[13] However, with gallbladder cancer's extremely poor prognosis, most patients will die within a year of surgery. If surgery is not possible, endoscopic stenting or percutaneous transhepatic biliary drainage (PTBD) of the biliary tree can reduce jaundice and a stent in the stomach may relieve vomiting. Chemotherapy and radiation may also be used with surgery. If gallbladder cancer is diagnosed after cholecystectomy for stone disease (incidental cancer), re-operation to remove part of liver and lymph nodes is required in most cases. When it is done as early as possible, patients have the best chance of long-term survival and even cure.[20]
Epidemiology
[edit]Most tumors are adenocarcinomas, with a small percent being squamous cell carcinomas.
- Gallbladder cancer is relatively rare, affecting fewer than 5000 people in the United States per year[21]
- Gallbladder cancer is more common in South American countries, Japan, and Israel; in Chile, gallbladder cancer is the fourth most common cause of cancer deaths.
- 5th most common gastrointestinal cancer
- Up to 5 times more common in women than men depending on population (e.g. 73% female in China) [22]
- The age adjusted incidence rates of gallbladder cancer is highest in Chile, followed by in the state of Assam in India[23]
Prognosis
[edit]The prognosis still remains poor. The cancer commonly spreads to the liver, bile duct, stomach, and duodenum.[24]
Research
[edit]A better understanding of the biology of biliary tract cancers, including gallbladder cancer, is being achieved by advances in genomic profiling.[25] This research is providing insight into deficiencies in the tumor cell's ability to accurately repair damages in their own DNA. The tumors in about 25% of patients with biliary tract cancer have some form of DNA damage repair deficiency.[25] Knowledge of such deficiencies can be exploited to potentially increase response to treatment strategies that are currently available such as chemotherapy, radiotherapy, or immunotherapy.
References
[edit]- ^ a b "Gallbladder cancer - Symptoms and causes". Mayo Clinic.
- ^ "Risk Factors for Gallbladder Cancer". www.cancer.org.
- ^ "Types of gallbladder cancer | Gallbladder cancer | Cancer Research UK".
- ^ "Gallbladder cancer - Diagnosis and treatment - Mayo Clinic". Mayo Clinic.
- ^ "Gallbladder Cancer - Statistics". 25 June 2012.
- ^ a b Henley, S. Jane; Weir, Hannah K.; Jim, Melissa A.; Watson, Meg; Richardson, Lisa C. (2015). "Gallbladder Cancer Incidence and Mortality, United States 1999–2011". Cancer Epidemiology, Biomarkers & Prevention. 24 (9): 1319–1326. doi:10.1158/1055-9965.EPI-15-0199. PMID 26070529. S2CID 886615.
- ^ Henley, S. Jane; Weir, Hannah K.; Jim, Melissa A.; Watson, Meg; Richardson, Lisa C. (2018-09-27). "CDC - Gallbladder Cancer Incidence and Death Rates". Cancer Epidemiology, Biomarkers & Prevention. 24 (9): 1319–1326. doi:10.1158/1055-9965.EPI-15-0199. PMID 26070529. S2CID 886615. Retrieved 2018-12-10.
- ^ Kapoor VK, McMichael AJ (2003). "Gallbladder cancer: an 'Indian' disease". Natl Med J India. 16 (4): 209–13. PMID 14606770.
- ^ Fitzgerald, J Edward F; White Matthew J; Lobo Dileep N (Apr 2009). "Courvoisier's gallbladder: law or sign?". World Journal of Surgery. 33 (4). United States: 886–91. doi:10.1007/s00268-008-9908-y. ISSN 0364-2313. PMID 19190960. S2CID 21799234.
- ^ Folseraas, T; Boberg, KM (February 2016). "Cancer Risk and Surveillance in Primary Sclerosing Cholangitis". Clinics in Liver Disease. 20 (1): 79–98. doi:10.1016/j.cld.2015.08.014. PMID 26593292.
- ^ Ferreccio, C. (2012). "Salmonella typhi and Gallbladder Cancer". Bacteria and Cancer. pp. 117–137. doi:10.1007/978-94-007-2585-0_5. ISBN 978-94-007-2584-3.
- ^ Srivastava K, Srivastava A, Sharma KL, Mittal B. Candidate gene studies in gallbladder cancer: a systematic review and meta-analysis. Mutat Res. 2011 Jul–Oct;728(1–2):67–79.
- ^ a b c d "Gallbladder Cancer: Symptoms, Causes & Treatment | Dr. Nikhil Agrawal". Dr.Nikhil Agrawal. Retrieved 2020-10-11.
- ^ Duffy, A.; Capanu, M.; Abou-Alfa, G. K.; Huitzil, D.; Jarnagin, W.; Fong, Y.; D'Angelica, M.; Dematteo, R. P.; Blumgart, L. H. (2008-12-01). "Gallbladder cancer (GBC): 10-year experience at Memorial Sloan-Kettering Cancer Centre (MSKCC)". Journal of Surgical Oncology. 98 (7): 485–489. doi:10.1002/jso.21141. ISSN 1096-9098. PMID 18802958. S2CID 43595860.
- ^ "Tests for gallbladder cancer". Cancer Research UK. Archived from the original on 10 October 2011. Retrieved 17 September 2012.
- ^ a b Makino I, Yamaguchi T, Sato N, Yasui T, Kita I (August 2009). "Xanthogranulomatous cholecystitis mimicking gallbladder carcinoma with a false-positive result on fluorodeoxyglucose PET". World J. Gastroenterol. 15 (29): 3691–3. doi:10.3748/wjg.15.3691. PMC 2721248. PMID 19653352.
- ^ Rao RV, Kumar A, Sikora SS, Saxena R, Kapoor VK (2005). "Xanthogranulomatous cholecystitis: differentiation from associated gall bladder carcinoma". Trop Gastroenterol. 26 (1): 31–3. PMID 15974235.
- ^ McCoy JJ, Vila R, Petrossian G, McCall RA, Reddy KS (March 1976). "Xanthogranulomatous cholecystitis. Report of two cases". J S C Med Assoc. 72 (3): 78–9. PMID 1063276.
- ^ "Cholecystectomy: Approaches and Technique". The Lecturio Medical Concept Library. Retrieved 8 July 2021.
- ^ "Gallbladder Cancer Treatment (PDQ®)–Patient Version". National Cancer Institute. 24 March 2004. Retrieved 8 July 2021.
- ^ Carriaga, M. T.; Henson, D. E. (1995-01-01). "Liver, gallbladder, extrahepatic bile ducts, and pancreas". Cancer. 75 (1 Suppl): 171–190. doi:10.1002/1097-0142(19950101)75:1+<171::AID-CNCR2820751306>3.0.CO;2-2. ISSN 0008-543X. PMID 8000995.[dead link]
- ^ Hsing AW, Gao YT, Han TQ, et al. (December 2007). "Gallstones and the risk of biliary tract cancer: a population-based study in China". Br. J. Cancer. 97 (11): 1577–82. doi:10.1038/sj.bjc.6604047. PMC 2360257. PMID 18000509.
- ^ National Cancer Registry Programme (2013).Three-year report of population based cancer registries:2009-2011. NCDIR-ICMR, Bangalore.
- ^ Goetze, T.O (21 November 2015). "Gallbladder carcinoma: Prognostic factors and therapeutic options". World Journal of Gastroenterology. 21 (43): 12211–12217. doi:10.3748/wjg.v21.i43.12211. PMC 4649107. PMID 26604631.
- ^ a b Lamarca A, Barriuso J, McNamara MG, Valle JW. Biliary Tract Cancer: State of the Art and potential role of DNA Damage Repair. Cancer Treat Rev. 2018 Nov;70:168-177. doi: 10.1016/j.ctrv.2018.09.002. Epub 2018 Sep 8. PMID 30218788
External links
[edit]| Authority control databases: National |
|---|