
Pudendal nerve
| Pudendal nerve | |
|---|---|
 Pudendal nerve, course and branches | |
 Sacral plexus of the right side (inferior pudendal labeled at bottom right). | |
| Details | |
| From | Sacral nerves S2-S4 |
| To | Inferior rectal nerves perineal nerve dorsal nerve of the penis |
| Identifiers | |
| Latin | Nervus pudendus |
| MeSH | D060525 |
| TA98 | A14.2.07.037 |
| TA2 | 6554 |
| FMA | 19037 |
| Anatomical terms of neuroanatomy | |
The pudendal nerve is a nerve in the pelvic region that carries sensory and motor, somatic and sympathetic[1][2] fibers that innervate the external genitalia of both sexes, as well as sphincters for the bladder and the rectum. It originates in Onuf's nucleus in the sacral region of the spinal cord, and travels in the S2-S4 nerves of the sacral plexus.
Anatomy
The pudendal nerve originates in the sacral plexus; it derives its fibers from the ventral rami of the second, third, and fourth sacral nerves (S2, S3, S4).[3]
It passes between the piriformis and coccygeus muscles and leaves the pelvis through the lower part of the greater sciatic foramen.
It crosses the spine of the ischium, and reenters the pelvis through the lesser sciatic foramen.
It accompanies the internal pudendal vessels upward and forward along the lateral wall of the ischiorectal fossa, being contained in a sheath of the obturator fascia termed the pudendal canal.
The pudendal nerve gives off the inferior rectal nerves. It soon divides into two terminal branches: the perineal nerve, and the dorsal nerve of the penis (in males) or the dorsal nerve of the clitoris (in females).
| Branch | Description |
| Inferior anal nerves | given off shortly after passing through the Greater sciatic foramen. |
| Perineal nerve | more superficial terminal branch |
| Dorsal nerve of penis/Dorsal nerve of clitoris | deeper terminal branch, traveling into the deep perineal pouch |
| Posterior scrotal nerves/Posterior labial nerves | Posterior scrotum/Posterior labia |
Research shows that variations in pudendal nerve origin are possible. For example, the pudendal nerve may actually originate off of the Sciatic nerve.[4] Consequently, damage to the sciatic nerve can affect the pudendal nerve as well.
Physiology
The pudendal nerve innervates the penis and clitoris, bulbospongiosus and ischiocavernosus muscles, and areas around the scrotum, perineum, and anus. Its postsynaptic sympathetic fibers innervate penile erectile tissue to induce tonic coiling of the helicine arteries of penis.
During erection, this coiling is inhibited by parasympathetic fibers of the cavernous nerves. At sexual climax, the spasms in the bulbospongiosus and ischiocavernous results in ejaculation in the male and most of the feelings of orgasm in both sexes.
Pathology
Difficult childbirth or bicycling[5] can compress or stretch the pudendal nerve, causing temporary loss of function, but permanent injury is rare. Entrapment of the nerve is very rare but can happen. A pelvic tumor (most notably a large sacrococcygeal teratoma), or surgery to remove the tumor, can damage this nerve permanently. A pudendal nerve block, also known as a saddle nerve block is a common obstetric procedure to anesthetize the perineum during labor.[6]
The pudendal nerve terminal motor latency test is a diagnostic procedure used to quantify the length of time it takes for the anal sphincter to respond to the electrical stimulus of the pudendal nerve using a St. Mark's electrode. Prolonged motor latency can be an indicator of the extent of idiopathic and childbirth related neurological damage to the pudendal nerve, and can provide some indication regarding potential recovery.
Radiology
The pudendal nerve is difficult to visualize on routine CT or MR imaging, however under CT guidance, a needle may be placed adjacent to the pudendal neurovascular bundle. The ischial spine, an easily identifiable structure on CT, is used as the level of injection. A spinal needle is advanced via the gluteal muscles and advanced within several millimeters of the ischial spine. Contrast (X-ray dye) is then injected, highlighting the nerve in the canal, confirming correct needle placement. The nerve may then be injected with cortisone and local anaesthetic to confirm and also treat chronic pain of the external genitalia (known as vulvodynia in females), pelvic and anorectal pain[7][8] In rare cases, the nerve may be destroyed with either alcoholic or radiofrequency ablation.
Additional images
-
 Dissection of side wall of pelvis showing sacral and pudendal plexuses. (Pudendal nerve labeled at center right.
Dissection of side wall of pelvis showing sacral and pudendal plexuses. (Pudendal nerve labeled at center right. -
 The superficial branches of the internal pudendal artery.
The superficial branches of the internal pudendal artery. -
 Plan of sacral and pudendal plexuses.
Plan of sacral and pudendal plexuses. -
 Schematic of sacral plexus with pudendal nerve shown in bottom right.
Schematic of sacral plexus with pudendal nerve shown in bottom right.




See also
References
- ^ Grant's atlas of anatomy 11th edition. pg 221
- ^ Knobil and Neill's Physiology of Reproduction, Volume 1. pg 1738
- ^ Moore, K.L., & Agur, A.M. (2007). Essential Clinical Anatomy: Third Edition. Baltimore: Lippincott Williams & Wilkins. 215. ISBN 978-0-7817-6274-8
- ^ Unusual origin of dorsal nerve of penis and abnormal formation of pudendal nerve—Clinical significance http://www.sciencedirect.com/science/article/pii/S0940960206000926
- ^ Mellion MB (1991). "Common cycling injuries. Management and prevention". Sports Med. 11 (1): 52–70. doi:10.2165/00007256-199111010-00004. PMID 2011683.
{{cite journal}}: Unknown parameter|month=ignored (help) - ^ Lynna Y. Littleton, Joan Engebretson (2002). Maternal, Neonatal, and Women's Health Nursing, Volume 1. Cengage Learning. p. 727.
- ^ Calvillo O, Skaribas IM, Rockett C. (2000). "Computed tomography-guided pudendal nerve block. A new diagnostic approach to long-term anoperineal pain: a report of two cases". Reg Anesth Pain Med. 24 (4): 420–3. doi:10.1053/rapm.2000.7620. PMID 10925942.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Hough DM, Wittenberg KH, Pawlina W, Maus TP, King BF, Vrtiska TJ, Farrell MA, Antolak SJ Jr. (2003). "Chronic perineal pain caused by pudendal nerve entrapment: anatomy and CT-guided perineural injection technique". Am J Roentgenol. 181 (2): 561–7. PMID 12876048.
{{cite journal}}: CS1 maint: multiple names: authors list (link)
External links
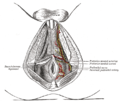
- Anatomy figure: 41:04-11 at Human Anatomy Online, SUNY Downstate Medical Center - "Inferior view of female perineum, branches of the internal pudendal artery."
- figures/chapter_32/32-2.HTM: Basic Human Anatomy at Dartmouth Medical School
- figures/chapter_32/32-3.HTM: Basic Human Anatomy at Dartmouth Medical School
- Diagnosis and treatment options, lists of doctors and physical therapists.
- Cross section image: pelvis/pelvis-female-17—Plastination Laboratory at the Medical University of Vienna
- Diagnosis and treatment at www.nervemed.com
- www.pudendal.com
- Pudendal nerve entrapment at chronicprostatitis.com
- CT sequence showing a pudendal nerve block.