
Rotator cuff: Difference between revisions
internal rotators 'unliked', broken link changed |
<ref> updated |
||
| Line 36: | Line 36: | ||
|} |
|} |
||
The [[mnemonic]] ''''SITS'''', sometimes written ''''SItS'''' as an additional hint that the teres minor is a member, is often used to remember the four muscles of the rotator cuff.<ref name="mnemonic">[http://mc.lifehugger.com/ |
The [[mnemonic]] ''''SITS'''', sometimes written ''''SItS'''' as an additional hint that the teres minor is a member, is often used to remember the four muscles of the rotator cuff.<ref name="mnemonic">[http://mc.lifehugger.com/moc/121/rotator-cuff-muscles Mnemonic for rotator cuff muscles.]</ref> |
||
==Injuries== |
==Injuries== |
||
Revision as of 08:44, 20 March 2009
| Rotator cuff | |
|---|---|
 Muscles on the dorsum of the scapula, and the Triceps brachii. | |
 The scapular and circumflex arteries. | |
| Identifiers | |
| MeSH | D017006 |
| TA2 | 2461 |
| FMA | 37018 |
| Anatomical terminology | |
The rotator cuff (rotor cuff) is an anatomical term given to the group of muscles and their tendons that act to stabilize the shoulder. Along with the teres major and the deltoid, the four muscles of the rotator cuff make up the six scapulohumeral (those that connect to the humerus and scapula and act on the glenohumeral joint) muscles of the human body.
Function
The rotator cuff muscles are important in shoulder movements and in maintaining glenohumeral joint (shoulder joint) stability. [1]These muscles arise from the scapula and connect to the head of the humerus forming a cuff at the shoulder joint. They hold the head of the humerus in the small and shallow glenoid fossa of the scapula. The glenohumeral joint is often likened to a golf ball(head of the humerus) sitting on a golf tee(glenoid fossa). During abduction of the arm, the rotator cuff compresses the glenohumeral joint in order to allow the large deltoid muscle to further elevate the arm. In other words, without the rotator cuff, the humeral head would ride up partially out of the glenoid fossa, lessening the efficiency of the deltoid muscle. During flexion of the arm infraspinatus and subscapularis act as joint stabilizers. During extension subscapularis and supraspinatus help stabilize the shoulder joint. Subscapularis stabilizes the joint during external rotation.[1]
Muscles composing rotator cuff
| Muscle | Origin on scapula | Attachment on humerus | Function | Innervation |
| Supraspinatus muscle | supraspinous fossa | greater tubercle | abducts the arm | Suprascapular nerve (C5) |
| Infraspinatus muscle | infraspinous fossa | greater tubercle | externally rotates the arm | Suprascapular nerve (C5-C6) |
| Teres minor muscle | lateral border | greater tubercle | externally rotates the arm | Axillary nerve (C5) |
| Subscapularis muscle | subscapular fossa | lesser tubercle | internally rotates the humerus | Subscapular nerve (C5-C6) |
The mnemonic 'SITS', sometimes written 'SItS' as an additional hint that the teres minor is a member, is often used to remember the four muscles of the rotator cuff.[2]
Injuries
Rotator cuff tear
The tendons at the ends of the rotator cuff muscles can become torn, leading to pain and restricted movement of the arm. A torn rotator cuff can occur following a trauma to the shoulder or it can occur through "wear and tear" of the tendons (most commonly that of the supraspinatus) under the acromion. It is an injury frequently sustained by athletes whose duties involve making repetitive throws, such as baseball pitchers, American football quarterbacks, volleyball (due to their swinging motions), water polo players, swimmers, boxers, kayaking, fast bowlers in cricket, and tennis players (due to their service motion). This type of injury also commonly affects conductors (music), choral conductor, orchestral conductor, due to the swinging motions and other movements used to lead their ensemble. It is commonly associated with motions that require repeated overhead motions or forceful pulling motions.
Rotator cuff impingement
A systematic review of relevant research found that the accuracy of the physical examination is low.[3] The Hawkins-Kennedy test[4][5] has a sensitivity of approximately 80% to 90% for detecting impingement. The infraspinatus and supraspinatus[6] tests have a specificity of 80% to 90%.[3]
Treatment
Reduce pain and swelling
As with all muscle injuries, R.I.C.E. is the modality recommended by physicians, DOs, physical therapists, athletic trainers, and chiropractors.[citation needed]
- Rest means ceasing movement of the affected area.
- Icing uses ice to reduce inflammation.
- Compression limits the swelling.
- Elevation involves placing the area higher to reduce inflammation and swelling.
Cold compression therapy is very useful for all muscle tears and strains as it reduces pain and swelling. Using a cold compression therapy wrap for 15 minutes before sleeping can aid in reducing the pain that causes restless sleep.[citation needed]
Strengthening
The rotator cuff can be strengthened to rehabilitate shoulder injuries, and prevent future ones. There are different exercises to target the individual rotator cuff muscles.
| Description | Beginning | End |
| The most effective is the side-lying external rotation, which activates the supraspinatus, subscapularis, infraspinatus and teres minor. The side-lying external rotation involves the person selecting a dumbbell of low weight initially when first training - no more than 3 kilograms. The lifter lies on a bench sideways, with the arm next to his side and flexed about 90 degrees at the elbow. Rotate the upper arm, raising the dumbbell towards the ceiling to a 45 degree angle, with the elbow still flexed and the upper arm close to the body, at a pace of two seconds up and four seconds down. This is an excellent all-round shoulder exercise. |  |

|
| Another exercise is the propped external rotator, which targets the infraspinatus and teres minor. The lifter should sit perpendicular to the barbell, with his arm flexed at 90 degrees at the elbow and the forearm resting parallel on the barbell. Again, selecting a dumbbell of modest weight if just beginning, raise the dumbbell up until the forearm points up. Slowly lower the dumbbell and repeat, exercising both arms. |  |

|
| The final exercise is the lateral raise with internal rotation (LRIR). Grasping a dumbbell in each hand, the lifter should internally rotate his arm so that his extended thumbs point towards the floor - as if the lifter is emptying a drink into a bin. The lifter should then raise his arms sideways, with the thumbs still pointing downwards, until the dumbbells are just below the shoulders. The LRIR primarily targets the supraspinatus. |  |

|
Strengthening the rotator cuff allows for increased loads in a variety of exercises. When weightlifters are unable to increase the weight they can lift on a pushing exercise (such as the bench press or military press) for an extended period of time, strengthening the rotator cuff can often allow them to begin making gains again. It also prevents future injuries to the glenohumeral joint, balancing the often-dominant internal rotators with stronger external rotators. Finally, exercising the rotator cuff can lead to improved posture, as without exercise to the external rotator, the internal rotators can see a shortening, leading to tightness. This often manifests itself as rounded shoulders in the population.
Surgery
Even for full thickness rotator cuff tears, conservative care outcomes are usually reasonable[7] However, many patients still suffer disability and pain despite non-surgical therapies. For massive tears of the rotator cuff, surgery has shown durable outcomes on 10 year follow-up.[8] However, the same study demonstrated ongoing and progressive fatty atrophy and re-tears of the rotator cuff. Shen has shown that MRI evidence of fatty atrophy in the rotator cuff prior to surgery is predicative of a poor surgical outcome.[9] To address this issue of failure of surgical repair and poor conservative care outcomes caused by muscular atrophy, bioengineering may be the answer. Mesenchymal stem cells have been shown to differentiate into skeletal muscle.[10] The first commercial applications that demonstrate rotator cuff repair on high field MRI using percutaneously implanted stem cells are just reaching the marketplace.[11] If the rotator cuff is completely torn, surgery is usually required to reattach the tendon to the bone.[1]
Additional images
-
 Diagram of the human shoulder joint
Diagram of the human shoulder joint -
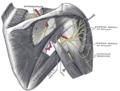 Suprascapular and axillary nerves of right side, seen from behind.
Suprascapular and axillary nerves of right side, seen from behind. -
 The suprascapular, axillary, and radial nerves.
The suprascapular, axillary, and radial nerves.



References
This article needs additional citations for verification. (June 2008) |
- ^ a b Morag, Yoav; Jacobson, Jon A.; Miller, Bruce; De Maeseneer, Michel; Girish, Gandikota; Jamadar, David (2006), "MR Imaging of Rotator Cuff Injury: What the Clinician Needs to Know", RadioGraphics, 26 (4): 1045, doi:10.1148/rg.264055087, PMID 16844931
- ^ Mnemonic for rotator cuff muscles.
- ^ a b Hegedus EJ, Goode A, Campbell S; et al. (2007). "Physical Examination Tests of the Shoulder: A Systematic Review with Meta-analysis of Individual Tests". British Journal of Sports Medicine. 42: 80. doi:10.1136/bjsm.2007.038406. PMID 17720798.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link) - ^ ShoulderDoc.co.uk Shoulder and Elbow Surgery. "Hawkins-Kennedy Test". Retrieved 2007-09-12. (video)
- ^ Brukner P, Khan K, Kibler WB. "Chapter 14: Shoulder Pain". Retrieved 2007-08-30.
{{cite web}}: CS1 maint: multiple names: authors list (link) - ^ ShoulderDoc.co.uk Shoulder and Elbow Surgery. "Empty Can/Full Can Test". Retrieved 2007-09-12. (video)
- ^ Baydar; et al. "The efficacy of conservative treatment in patients with full-thickness rotator cuff tears". PubMed.
{{cite web}}: Explicit use of et al. in:|author=(help) - ^ Zumstein; et al. "IThe clinical and structural long-term results of open repair of massive tears of the rotator cuff". PubMed.
{{cite web}}: Explicit use of et al. in:|author=(help) - ^ Shen; et al. "Long-term functional outcomes after repair of rotator cuff tears correlated with atrophy of the supraspinatus muscles on magnetic resonance images". PubMed.
{{cite web}}: Explicit use of et al. in:|author=(help) - ^ {{| author=Arthur et al| publisher=PubMed | title=The therapeutic applications of multipotential mesenchymal/stromal stem cells in skeletal tissue repair.|http://www.ncbi.nlm.nih.gov/pubmed/18792913?ordinalpos=7&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DefaultReportPanel.Pubmed_RVDocSum }}
- ^ "Percutaneous mesenchymal stem cell based procedure". Regenerative Sciences.