
Aspergillosis
| Aspergillosis | |
|---|---|
| Specialty | Infectious disease |
Aspergillosis is the name given to a wide variety of diseases caused by infection by fungi of the genus Aspergillus. The majority of cases occur in people with underlying illnesses such as tuberculosis[1] or chronic obstructive pulmonary disease (COPD), but with otherwise healthy immune systems.[2] Most commonly, aspergillosis occurs in the form of chronic pulmonary aspergillosis (CPA), aspergilloma or allergic bronchopulmonary aspergillosis (ABPA).[3] Some forms are intertwined; for example ABPA and simple aspergilloma can progress to CPA.
Other, non-invasive manifestations include fungal sinusitis (both allergic in nature and with established fungal balls), otomycosis (ear infection), keratitis (eye infection) and onychomycosis (nail infection). In most instances these are less severe, and curable with effective antifungal treatment.
People with deficient immune systems—such as patients undergoing hematopoietic stem cell transplantation, chemotherapy for leukaemia, or AIDS—are at risk of more disseminated disease. Acute invasive aspergillosis occurs when the immune system fails to prevent Aspergillus spores from entering the bloodstream via the lungs. Without the body mounting an effective immune response, fungal cells are free to disseminate throughout the body and can infect major organs such as the heart and kidneys.
The most frequently identified pathogen is Aspergillus fumigatus—a ubiquitous organism that is capable of living under extensive environmental stress. It is estimated that most humans inhale thousands of Aspergillus spores daily, but they do not affect most people’s health due to effective immune responses. Taken together, the major chronic, invasive and allergic forms of aspergillosis account for around 600,000 deaths annually worldwide.[1]Cite error: The <ref> tag has too many names (see the help page).Cite error: The <ref> tag has too many names (see the help page).Cite error: The <ref> tag has too many names (see the help page).Cite error: The <ref> tag has too many names (see the help page).
Symptoms
A fungus ball in the lungs may cause no symptoms and may be discovered only with a chest X-ray, or it may cause repeated coughing up of blood, chest pain, and occasionally severe, even fatal, bleeding. A rapidly invasive Aspergillus infection in the lungs often causes cough, fever, chest pain, and difficulty breathing.
Poorly controlled aspergillosis can disseminate through the blood stream to cause widespread organ damage. Symptoms include fever, chills, shock, delirium, seizures and blood clots. The person may develop kidney failure, liver failure (causing jaundice), and breathing difficulties. Death can occur quickly.
Aspergillosis of the ear canal causes itching and occasionally pain. Fluid draining overnight from the ear may leave a stain on the pillow. Aspergillosis of the sinuses causes a feeling of congestion and sometimes pain or discharge. It can extend beyond the sinuses.[4]
In addition to the symptoms, an X-ray or computerised tomography (CT) scan of the infected area provides clues for making the diagnosis. Whenever possible, a doctor sends a sample of infected material to a laboratory to confirm identification of the fungus.
Diagnosis
On chest X-ray and CT, pulmonary aspergillosis classically manifests as a halo sign, and, later, an air crescent sign.[5] In hematologic patients with invasive aspergillosis, the galactomannan test can make the diagnosis in a noninvasive way. False positive Aspergillus Galactomannan tests have been found in patients on intravenous treatment with some antibiotics or fluids containing gluconate or citric acid such as some transfusion platelets, parenteral nutrition or PlasmaLyte
On microscopy, Aspergillus species are reliably demonstrated by silver stains, e.g., Gridley stain or Gomori methenamine-silver.[6] These give the fungal walls a gray-black colour. The hyphae of Aspergillus species range in diameter from 2.5 to 4.5 µm. They have septate hyphae,[7] but these are not always apparent, and in such cases they may be mistaken for Zygomycota.[6] Aspergillus hyphae tend to have dichotomous branching that is progressive and primarily at acute angles of about 45°.[6]
-
 Angio invasive pulmonary aspergillosis
Angio invasive pulmonary aspergillosis -
 Angio invasive pulmonary aspergillosis (closeup)
Angio invasive pulmonary aspergillosis (closeup) -
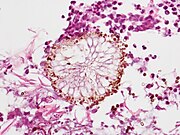 Aspergillus vesicle (HE stain).
Aspergillus vesicle (HE stain).

_invasive_type.jpg)

Treatment
The current medical treatments for aggressive invasive Aspergillosis include voriconazole and liposomal amphotericin B in combination with surgical debridement.[8] For the less aggressive allergic bronchopulmonary aspergillosis findings suggest the use of oral steroids for a prolonged period of time, preferably for 6–9 months in allergic aspergillosis of the lungs. Itraconazole is given with the steroids, as it is considered to have a "steroid sparing" effect, causing the steroids to be more effective, allowing a lower dose.,[9]
Other drugs used, such as amphotericin B, caspofungin (in combination therapy only), flucytosine (in combination therapy only), or itraconazole,[10][11] are used to treat this fungal infection. However, a growing proportion of infections are resistant to the triazoles.[12] A. fumigatus, the most commonly infecting species, is intrinsically resistant to fluconazole.[13]
Prevention
Prevention of Aspergillosis involves a reduction of mold exposure via environmental infection-control. Anti-fungal prophylaxis can be given to high-risk patients. Posaconazole is often given as prophylaxis in severely immunocompromised patients.[14]
Infections in animals
Albeit relatively rare in humans, aspergillosis is a common and dangerous infection in birds, particularly in pet parrots. Mallards and other ducks are particularly susceptible, as they will often resort to poor food sources during bad weather. Captive raptors, such as falcons and hawks, are susceptible to this disease if they are kept in poor conditions and especially if they are fed pigeons, which are often carriers of "asper". It can be acute in chicks, but chronic in mature birds.
Aspergillosis has been the culprit in several rapid die-offs among waterfowl. From 8 December until 14 December 2006, over 2,000 Mallards died in the Burley, Idaho area of the USA, an agricultural community approximately 150 miles southeast of Boise. Mouldy waste grain from the farmland and feedlots in the area is the suspected source. A similar aspergillosis outbreak caused by mouldy grain killed 500 Mallards in Iowa, USA, in 2005.
While there is no connection between aspergillosis and the H5N1 strain of avian influenza (commonly called "bird flu"), rapid die-offs caused by aspergillosis can spark fears of bird flu outbreaks. Laboratory analysis is the only way to distinguish bird flu from aspergillosis.
In dogs, aspergillosis is an uncommon disease typically affecting only the nasal passages (nasal aspergillosis). This is much more common in dolicocephalic breeds. It can also spread to the rest of the body; this is termed disseminated aspergillosis and is rare, usually affecting individuals with underlying immune disorders.
See also
References
- ^ a b Denning, D. W.; Pleuvry, A.; Cole, D. C. (March 2013). "Global burden of chronic pulmonary aspergillosis complicating sarcoidosis". European Respiratory Journal. 41 (3): 621–6. doi:10.1183/09031936.00226911. PMID 22743676.
- ^ Smith, N; Denning, D.W. (1 April 2011). "Underlying conditions in chronic pulmonary aspergillosis including simple aspergilloma". European Respiratory Journal. 37 (4): 865–872. doi:10.1183/09031936.00054810. PMID 20595150.
- ^ Goel, Ayush. "Pulmonary aspergillosis". Mediconotebook. Retrieved 29 May 2015.
- ^ Ederies A, Chen J, Aviv RI; et al. (May 2010). "Aspergillosis of the Petrous Apex and Meckel's Cave". Skull Base. 20 (3): 189–92. doi:10.1055/s-0029-1246229. PMC 3037105. PMID 21318037.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Curtis A, Smith G, Ravin C (1 October 1979). "Air crescent sign of invasive aspergillosis". Radiology. 133 (1): 17–21. doi:10.1148/133.1.17. PMID 472287.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ a b c Kradin RL, Mark EJ (April 2008). "The pathology of pulmonary disorders due to Aspergillus spp". Arch. Pathol. Lab. Med. 132 (4): 606–14. doi:10.1043/1543-2165(2008)132[606:TPOPDD]2.0.CO;2. PMID 18384212.
- ^ "Mycoses: Aspergillosis". Mycology Online. Archived from the original on 7 December 2008. Retrieved 2008-12-10.
{{cite web}}: Unknown parameter|deadurl=ignored (|url-status=suggested) (help) - ^ Kontoyiannis, Dimitrios P.; Lionakis, Michail S.; Lewis, Russell E.; Chamilos, Georgios; Healy, Mimi; Perego, Cheryl; Safdar, Amar; Kantarjian, Hagop; Champlin, Richard; Walsh, Thomas J.; Raad, Issam I. (2005). "Zygomycosis in a Tertiary‐Care Cancer Center in the Era ofAspergillus‐Active Antifungal Therapy: A Case‐Control Observational Study of 27 Recent Cases". The Journal of Infectious Diseases. 191 (8): 1350–1360. doi:10.1086/428780. ISSN 0022-1899.
- ^ Walsh TJ, Anaissie EJ, Denning DW; et al. (February 2008). "Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America". Clin. Infect. Dis. 46 (3): 327–60. doi:10.1086/525258. PMID 18177225.
{{cite journal}}: CS1 maint: multiple names: authors list (link) As PDF - ^ Herbrecht R, Denning D, Patterson T, Bennett J, Greene R, Oestmann J, Kern W, Marr K, Ribaud P, Lortholary O, Sylvester R, Rubin R, Wingard J, Stark P, Durand C, Caillot D, Thiel E, Chandrasekar P, Hodges M, Schlamm H, Troke P, de Pauw B; Invasive Fungal Infections Group of the European Organisation for Research and Treatment of Cancer and the Global Aspergillus Study Group. (8 August 2002). "Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis". N Engl J Med. 347 (6): 408–15. doi:10.1056/NEJMoa020191. PMID 12167683.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Cornely OA, Maertens J, Bresnik M; et al. (May 2007). "Liposomal amphotericin B as initial therapy for invasive mold infection: a randomized trial comparing a high-loading dose regimen with standard dosing (AmBiLoad trial)". Clin. Infect. Dis. 44 (10): 1289–97. doi:10.1086/514341. PMID 17443465.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Denning DW, Park S, Lass-Florl C, Fraczek MG, Kirwan M, Gore R, Smith J, Bueid A, Bowyer P, Perlin DS (2011). "High-frequency Triazole Resistance Found In Nonculturable Aspergillus fumigatus from Lungs of Patients with Chronic Fungal Disease". Clin Infect Dis. 52 (9): 1123–9. doi:10.1093/cid/cir179. PMC 3106268. PMID 21467016.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Perea, S; Patterson, TF (1 November 2002). "Antifungal resistance in pathogenic fungi". Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 35 (9): 1073–80. doi:10.1086/344058. PMID 12384841. Retrieved 14 January 2015.
- ^ Cornely, Oliver A.; Maertens, Johan; Winston, Drew J.; Perfect, John; Ullmann, Andrew J.; Walsh, Thomas J.; Helfgott, David; Holowiecki, Jerzy; Stockelberg, Dick; Goh, Yeow-Tee; Petrini, Mario; Hardalo, Cathy; Suresh, Ramachandran; Angulo-Gonzalez, David (2007). "Posaconazole vs. Fluconazole or Itraconazole Prophylaxis in Patients with Neutropenia". New England Journal of Medicine. 356 (4): 348–359. doi:10.1056/NEJMoa061094. ISSN 0028-4793. PMID 17251531.
External links
- USGS National Wildlife Health Center
- Aspergillus — Aspergillus website
- Aspergillosis The National Aspergillosis Centre, UK
- Aspergillus The Aspergillus Website Blog
- Aspergillosis at DoctorFungus.org
- Adetunji, Jo (13 June 2008). "Man dies after inhaling fungal spores from garden compost". The Guardian.
- Aspergillosis at Backyard Poultry