
Thyroid
| thyroid | |
|---|---|
 Thyroid and parathyroid. | |
| Details | |
| Precursor | Thyroid diverticulum (an extension of endoderm into 2nd Branchial arch) |
| System | Endocrine system |
| Identifiers | |
| Latin | glandula thyroidea |
| MeSH | D013961 |
| TA98 | A11.3.00.001 |
| TA2 | 3863 |
| FMA | 9603 |
| Anatomical terminology | |
The thyroid gland or simply, the thyroid /ˈθaɪərɔɪd/, in vertebrate anatomy, is one of the largest endocrine glands. The thyroid gland is found in the neck, below the thyroid cartilage (which forms the laryngeal prominence, or "Adam's apple"). The isthmus (the bridge between the two lobes of the thyroid) is located inferior to the cricoid cartilage.
The thyroid gland controls how quickly the body uses energy, makes proteins, and controls how sensitive the body is to other hormones. It participates in these processes by producing thyroid hormones, the principal ones being triiodothyronine (T3) and thyroxine which can sometimes be referred to as tetraiodothyronine (T4). These hormones regulate the rate of metabolism and affect the growth and rate of function of many other systems in the body. T3 and T4 are synthesized from both iodine and tyrosine. The thyroid also produces calcitonin, which plays a role in calcium homeostasis.
Hormonal output from the thyroid is regulated by thyroid-stimulating hormone (TSH) produced by the anterior pituitary, which itself is regulated by thyrotropin-releasing hormone (TRH) produced by the hypothalamus.
The thyroid gets its name from the Greek word for "shield", due to the shape of the related thyroid cartilage. The most common problems of the thyroid gland consist of an overactive thyroid gland, referred to as hyperthyroidism, and an underactive thyroid gland, referred to as hypothyroidism.
Anatomy

The thyroid gland is a butterfly-shaped organ and is composed of two cone-like lobes or wings, lobus dexter (right lobe) and lobus sinister (left lobe), connected via the isthmus. The organ is situated on the anterior side of the neck, lying against and around the larynx and trachea, reaching posteriorly the oesophagus and carotid sheath. It starts cranially at the oblique line on the thyroid cartilage (just below the laryngeal prominence, or 'Adam's Apple'), and extends inferiorly to approximately the fifth or sixth tracheal ring.[1] It is difficult to demarcate the gland's upper and lower border with vertebral levels because it moves position in relation to these during swallowing.
The thyroid gland is covered by a fibrous sheath, the capsula glandulae thyroidea, composed of an internal and external layer. The external layer is anteriorly continuous with the lamina pretrachealis fasciae cervicalis and posteriorolaterally continuous with the carotid sheath. The gland is covered anteriorly with infrahyoid muscles and laterally with the sternocleidomastoid muscle also known as sternomastoid muscle. On the posterior side, the gland is fixed to the cricoid and tracheal cartilage and cricopharyngeus muscle by a thickening of the fascia to form the posterior suspensory ligament of Berry.[2][3] The thyroid gland's firm attachment to the underlying trachea is the reason behind its movement with swallowing.[4] In variable extent, Lalouette's Pyramid, a pyramidal extension of the thyroid lobe, is present at the most anterior side of the lobe. In this region, the recurrent laryngeal nerve and the inferior thyroid artery pass next to or in the ligament and tubercle.
Between the two layers of the capsule and on the posterior side of the lobes, there are on each side two parathyroid glands.
The thyroid isthmus is variable in presence and size, can change shape and size, and can encompass a cranially extending pyramid lobe (lobus pyramidalis or processus pyramidalis), remnant of the thyroglossal duct. The thyroid is one of the larger endocrine glands, weighing 2-3 grams in neonates and 18-60 grams in adults, and is increased in pregnancy.
The thyroid is supplied with arterial blood from the superior thyroid artery, a branch of the external carotid artery, and the inferior thyroid artery, a branch of the thyrocervical trunk, and sometimes by the thyroid ima artery, branching directly from the brachiocephalic trunk. The venous blood is drained via superior thyroid veins, draining in the internal jugular vein, and via inferior thyroid veins, draining via the plexus thyroideus impar in the left brachiocephalic vein.
Lymphatic drainage passes frequently the lateral deep cervical lymph nodes and the pre- and parathracheal lymph nodes. The gland is supplied by parasympathetic nerve input from the superior laryngeal nerve and the recurrent laryngeal nerve.
Evolution
Phylogenetically, thyroid cells are derived from primitive iodide-concentrating gastroenteric cells. Given the essential nature of iodine compounds in living organisms, organisms moving from iodine-rich seas to iodine-deficient land needed stronger systems for uptake and storage of that element. The thyroid appears to have evolved to serve that need. Venturi et al.[5] suggested that iodide has an ancestral antioxidant function in all iodide-concentrating cells from primitive algae to more recent vertebrates. In 2008, this ancestral antioxidant action of iodides has been experimentally confirmed by Küpper et al.[6] Thyroxine has a 700 million year history. It is present, while showing no hormonal action, in the fibrous exoskeletal scleroproteins of the lowest invertebrates, Porifera and Anthozoa. The active hormone, triiodothyronine (T3), became active in metamorphosis and thermogenesis, allowing for better adaptation of organisms to terrestrial environment (fresh water, atmosphere, gravity, temperature and diet).
Embryological development
In the fetus[clarification needed], at 3–4 weeks of gestation, the thyroid gland appears as an epithelial proliferation in the floor of the pharynx at the base of the tongue between the tuberculum impar and the copula linguae at a point later indicated by the foramen cecum. The thyroid then descends in front of the pharyngeal gut as a bilobed diverticulum through the thyroglossal duct. Over the next few weeks, it migrates to the base of the neck, passing anterior to the hyoid bone. During migration, the thyroid remains connected to the tongue by a narrow canal, the thyroglossal duct.
Thyrotropin-releasing hormone (TRH) and thyroid-stimulating hormone (TSH) start being secreted from the fetal hypothalamus and pituitary at 18-20 weeks of gestation, and fetal production of thyroxine (T4) reach a clinically significant level at 18–20 weeks.[7] Fetal triiodothyronine (T3) remains low (less than 15 ng/dL) until 30 weeks of gestation, and increases to 50 ng/dL at term.[7] Fetal self-sufficiency of thyroid hormones protects the fetus against e.g. brain development abnormalities caused by maternal hypothyroidism.[8] However, preterm births can suffer neurodevelopmental disorders due to lack of maternal thyroid hormones due their own thyroid being insufficiently developed to meet their postnatal needs.[9]
The portion of the thyroid containing the parafollicular C cells, those responsible for the production of calcitonin, are derived from the neural crest. This is first seen as the ultimobranchial body, which joins the primordial thyroid gland during its descent to its final location in the anterior neck.
Aberrations in embryological development can cause various forms of thyroid dysgenesis.

Histology
At the microscopic level, there are three primary features of the thyroid:[10]
| Feature | Description |
| Follicles | The thyroid is composed of spherical follicles that selectively absorb iodine (as iodide ions, I-) from the blood for production of thyroid hormones, but also for storage of iodine in thyroglobulin, in fact iodine is necessary for other important iodine-concentrating organs as breast, stomach, salivary glands, thymus etc. (see iodine in biology).
Twenty-five percent of all the body's iodide ions are in the thyroid gland. Inside the follicles, colloid serves as a reservoir of materials for thyroid hormone production and, to a lesser extent, acts as a reservoir for the hormones themselves. Colloid is rich in a protein called thyroglobulin. |
| Thyroid epithelial cells (or "follicular cells") |
The follicles are surrounded by a single layer of thyroid epithelial cells, which secrete T3 and T4. When the gland is not secreting T3/T4 (inactive), the epithelial cells range from low columnar to cuboidal cells. When active, the epithelial cells become tall columnar cells. |
| Parafollicular cells (or "C cells") |
Scattered among follicular cells and in spaces between the spherical follicles are another type of thyroid cell, parafollicular cells, which secrete calcitonin. |
Physiology
The primary function of the thyroid is production of the hormones triiodothyronine (T3), thyroxine (T4), and calcitonin. Up to 80% of the T4 is converted to T3 by peripheral organs such as the liver, kidney and spleen. T3 is several times more powerful than T4, which is largely a prohormone, perhaps four[11] or even ten times more active.[12]
T3 and T4 production and action


- Thyroglobulin is synthesized in the rough endoplasmic reticulum and follows the secretory pathway to enter the colloid in the lumen of the thyroid follicle by exocytosis.
- Meanwhile, a sodium-iodide (Na/I) symporter pumps iodide (I-) actively into the cell, which previously has crossed the endothelium by largely unknown mechanisms.
- This iodide enters the follicular lumen from the cytoplasm by the transporter pendrin, in a purportedly passive manner.[15]
- In the colloid, iodide (I-) is oxidized to iodine (I0) by an enzyme called thyroid peroxidase.
- Iodine (I0) is very reactive and iodinates the thyroglobulin at tyrosyl residues in its protein chain (in total containing approximately 120 tyrosyl residues).
- In conjugation, adjacent tyrosyl residues are paired together.
- The entire complex re-enters the follicular cell by endocytosis.
- Proteolysis by various proteases liberates thyroxine and triiodothyronine molecules, which enters the blood by largely unknown mechanisms.
Thyroxine (T4) is synthesised by the follicular cells from free tyrosine and on the tyrosine residues of the protein called thyroglobulin (Tg). Iodine is captured with the "iodine trap" by the hydrogen peroxide generated by the enzyme thyroid peroxidase (TPO)[16] and linked to the 3' and 5' sites of the benzene ring of the tyrosine residues on Tg, and on free tyrosine. Upon stimulation by the thyroid-stimulating hormone (TSH), the follicular cells reabsorb Tg and cleave the iodinated tyrosines from Tg in lysosomes, forming T4 and T3 (in T3, one iodine atom is absent compared to T4), and releasing them into the blood. Deiodinase enzymes convert T4 to T3.[17] Thyroid hormone secreted from the gland is about 80-90% T4 and about 10-20% T3.[11][12]
Cells of the developing brain are a major target for the thyroid hormones T3 and T4. Thyroid hormones play a particularly crucial role in brain maturation during fetal development.[18] A transport protein that seems to be important for T4 transport across the blood–brain barrier (OATP1C1) has been identified.[19] A second transport protein (MCT8) is important for T3 transport across brain cell membranes.[19]
Non-genomic actions of T4 are those that are not initiated by liganding of the hormone to intranuclear thyroid receptor. These may begin at the plasma membrane or within cytoplasm. Plasma membrane-initiated actions begin at a receptor on the integrin alphaV beta3 that activates ERK1/2. This binding culminates in local membrane actions on ion transport systems such as the Na(+)/H(+) exchanger or complex cellular events including cell proliferation. These integrins are concentrated on cells of the vasculature and on some types of tumor cells, which in part explains the proangiogenic effects of iodothyronines and proliferative actions of thyroid hormone on some cancers including gliomas. T4 also acts on the mitochondrial genome via imported isoforms of nuclear thyroid receptors to affect several mitochondrial transcription factors. Regulation of actin polymerization by T4 is critical to cell migration in neurons and glial cells and is important to brain development.
T3 can activate phosphatidylinositol 3-kinase by a mechanism that may be cytoplasmic in origin or may begin at integrin alpha V beta3.
In the blood, T4 and T3 are partially bound to thyroxine-binding globulin (TBG), transthyretin, and albumin. Only a very small fraction of the circulating hormone is free (unbound) - T4 0.03% and T3 0.3%. Only the free fraction has hormonal activity. As with the steroid hormones and retinoic acid, thyroid hormones cross the cell membrane and bind to intracellular receptors (α1, α2, β1 and β2), which act alone, in pairs or together with the retinoid X-receptor as transcription factors to modulate DNA transcription[1].
T3 and T4 regulation
The production of thyroxine and triiodothyronine is regulated by thyroid-stimulating hormone (TSH), released by the anterior pituitary. The thyroid and thyrotropes form a negative feedback loop: TSH production is suppressed when the T4 levels are high.[20] The TSH production itself is modulated by thyrotropin-releasing hormone (TRH), which is produced by the hypothalamus and secreted at an increased rate in situations such as cold exposure (to stimulate thermogenesis). TSH production is blunted by somatostatin (SRIH), rising levels of glucocorticoids and sex hormones (estrogen and testosterone), and excessively high blood iodide concentration.
An additional hormone produced by the thyroid contributes to the regulation of blood calcium levels. Parafollicular cells produce calcitonin in response to hypercalcemia. Calcitonin stimulates movement of calcium into bone, in opposition to the effects of parathyroid hormone (PTH). However, calcitonin seems far less essential than PTH, as calcium metabolism remains clinically normal after removal of the thyroid (thyroidectomy), but not the parathyroids.
Disorders
Thyroid disorders include hyperthyroidism (abnormally increased activity), hypothyroidism (abnormally decreased activity) and thyroid nodules, which are generally benign thyroid neoplasms, but may be thyroid cancers. All these disorders may give rise to goiter, that is, an enlarged thyroid.
Hyperthyroidism
Hyperthyroidism, or overactive thyroid, is the overproduction of the thyroid hormones T3 and T4, and is most commonly caused by the development of Graves' disease,[citation needed] an autoimmune disease in which antibodies are produced which stimulate the thyroid to secrete excessive quantities of thyroid hormones. The disease can result in the formation of a toxic goiter as a result of thyroid growth in response to a lack of negative feedback mechanisms. It presents with symptoms such as a thyroid goiter, protruding eyes (exopthalmos), palpitations, excess sweating, diarrhea, weight loss, muscle weakness and unusual sensitivity to heat. The appetite is often increased.
Beta blockers are used to decrease symptoms of hyperthyroidism such as increased heart rate, tremors, anxiety and heart palpitations, and anti-thyroid drugs are used to decrease the production of thyroid hormones, in particular, in the case of Graves' disease. These medications take several months to take full effect and have side-effects such as skin rash or a drop in white blood cell count, which decreases the ability of the body to fight off infections. These drugs involve frequent dosing (often one pill every 8 hours) and often require frequent doctor visits and blood tests to monitor the treatment, and may sometimes lose effectiveness over time. Due to the side-effects[clarification needed] and inconvenience of such drug regimens, some patients choose to undergo radioactive iodine-131 treatment. Radioactive iodine is administered in order to destroy a proportion of or the entire thyroid gland, since the radioactive iodine is selectively taken up by the gland and gradually destroys the cells of the gland. Alternatively, the gland may be partially or entirely removed surgically, though iodine treatment is usually preferred since the surgery is invasive and carries a risk of damage to the parathyroid glands or the nerves controlling the vocal cords. If the entire thyroid gland is removed, hypothyroidism results.[21]
Hypothyroidism
Hypothyroidism is the underproduction of the thyroid hormones T3 and T4. Hypothyroid disorders may occur as a result of congenital thyroid abnormalities (see congenital hypothyroidism), autoimmune disorders such as Hashimoto's thyroiditis, iodine deficiency (more likely in poorer countries) or the removal of the thyroid following surgery to treat severe hyperthyroidism and/or thyroid cancer. Typical symptoms are abnormal weight gain, tiredness, baldness, cold intolerance, and bradycardia. Hypothyroidism is treated with hormone replacement therapy, such as levothyroxine, which is typically required for the rest of the patient's life. Thyroid hormone treatment is given under the care of a physician and may take a few weeks to become effective.[22]
Negative feedback mechanisms result in growth of the thyroid gland when thyroid hormones are being produced in sufficiently low quantities as a means of increasing the thyroid output; however, where the hypothyroidism is caused by iodine insufficiency, the thyroid is unable to produce T3 and T4 and as a result, the thyroid may continue to grow to form a non-toxic goiter. It is termed non-toxic as it does not produce toxic quantities of thyroid hormones, despite its size.
Initial hyperthyroidism followed by hypothyroidism
This is the overproduction of T3 and T4 followed by the underproduction of T3 and T4. There are two types: Hashimoto's thyroiditis and postpartum thyroiditis.
Hashimoto's thyroiditis or Hashimoto's Disease is an autoimmune disorder whereby the body's own immune system reacts with the thyroid tissues in an attempt to destroy it. At the beginning, the gland may be overactive, and then becomes underactive as the gland is damaged resulting in too little thyroid hormone production or hypothyroidism. Some patients may experience "swings" in hormone levels that can progress rapidly from hyper-to-hypothyroid (sometimes mistaken as severe moodswings, or even being bipolar, before the proper clinical diagnosis is made). Some patients may experience these "swings" over a longer period of time, over days or weeks or even months. Hashimoto's is more common in females than males, usually appearing after the age of 30, and tends to run in families meaning it can be seen as a genetic disease. Also more common in individuals with Hashimoto's Thyroiditis are type 1 diabetes and celiac disease.[23]
Postpartum thyroiditis occurs in some females following the birth of a child. After delivery, the gland becomes inflamed and the condition initially presents with overactivity of the gland followed by underactivity. In some cases, the gland may recover with time and resume its functions. In others it may not. The etiology is not always known, but can sometimes be attributed to autoimmunity, such as Hashimoto's Thyroiditis or Graves' Disease.
Cancers
In most cases, the thyroid cancer presents as a painless mass in the neck. It is very unusual for the thyroid cancers to present with symptoms, unless it has been neglected. One may be able to feel a hard nodule in the neck. Diagnosis is made using a needle biopsy and various radiological studies.[24]
Non-cancerous nodules
Many individuals may find the presence of thyroid nodules in the neck. The majority of these thyroid nodules are benign (non cancerous). The presence of a thyroid nodule does not mean that one has thyroid disease. Most thyroid nodules do not cause any symptoms, and most are discovered on an incidental examination. Doctors usually perform a needle aspiration biopsy of the thyroid to determine the status of the nodules. If the nodule is found to be non-cancerous, no other treatment is required. If the nodule is suspicious then surgery is recommended.
Congenital anomalies
A persistent thyroglossal duct or cyst is the most common clinically significant congenital anomaly of the thyroid gland. A persistent sinus tract may remain as a vestigial remnant of the tubular development of the thyroid gland. Parts of this tube may be obliterated, leaving small segments to form cysts. These occur at any age and might not become evident until adult life. Mucinous, clear secretions may collect within these cysts to form either spherical masses or fusiform swellings, rarely larger than 2 to 3 cm in diameter. These are present in the midline of the neck anterior to the trachea. Segments of the duct and cysts that occur high in the neck are lined by stratified squamous epithelium, which is essentially identical to that covering the posterior portion of the tongue in the region of the foreamen cecum. The anomalies that occur in the lower neck more proximal to the thyroid gland are lined by epithelium resembling the thyroidal acinar epithelium. Characteristically, next to the lining epithelium, there is an intense lymphocytic inflitrate. Superimposed infection may convert these lesions into abscess cavities, and rarely, give rise to cancers.[citation needed]
Other disorders
- Limited research shows that seasonal allergies may trigger episodes of hypo- or hyperthyroidism.[25][26]
- A ectopic thyroid is an entire or parts of the thyroid located in another part of the body than what is the usual case.
Thyroid function tests
| Test | Abbreviation | Normal ranges[27] |
|---|---|---|
| Serum thyrotropin/thyroid-stimulating hormone | TSH | 0.3–3.0 μU/ml |
| Free thyroxine | FT4 | 7–18 ng/l = 0.7–1.8 ng/dl |
| Serum triiodothyronine | T3 | 0.8–1.8 μg/l = 80–180 ng/dl |
| Radioactive iodine-123 uptake | RAIU | 10–30% |
| Radioiodine scan (gamma camera) | N/A | N/A - thyroid contrasted images |
| Free thyroxine fraction | FT4F | 0.03–0.005% |
| Serum thyroxine | T4 | 46–120 μg/l = 4.6–12.0 μg/dl |
| Thyroid hormone binding ratio | THBR | 0.9–1.1 |
| Free thyroxine index | FT4I | 4–11 |
| Free triiodothyronine l | FT3 | 230–619 pg/d |
| Free T3 Index | FT3I | 80–180 |
| Thyroxine-binding globulin | TBG | 12–20 ug/dl T4 +1.8 μg |
| TRH stimulation test | Peak TSH | 9–30 μIU/ml at 20–30 min. |
| Serum thyroglobulin l | Tg | 0-30 ng/m |
| Thyroid microsomal antibody titer | TMAb | Varies with method |
| Thyroglobulin antibody titer | TgAb | Varies with method |
- μU/ml = mU/l, microunit per milliliter
- ng/dl, nanograms per deciliter
- μg, micrograms
- pg/d, picograms per day
- μIU/ml = mIU/l, micro-international unit per milliliter
- See [2] for more information on medical units of measure
Significance of iodine
In areas of the world where iodine is lacking in the diet, the thyroid gland can become considerably enlarged, a condition called endemic goiter. Pregnant women on a diet that is severely deficient of iodine can give birth to infants who can present with thyroid hormone deficiency (congenital hypothyroidism), manifesting in problems of physical growth and development as well as brain development (a condition referred to as endemic cretinism). In many developed countries, newborns are routinely tested for congenital hypothyroidism as part of newborn screening. Children with congenital hypothyroidism are treated supplementally with levothyroxine, which facilitates normal growth and development.
Thyroxine is critical to the regulation of metabolism and growth throughout the animal kingdom. Among amphibians, for example, administering a thyroid-blocking agent such as propylthiouracil (PTU) can prevent tadpoles from metamorphosing into frogs; in contrast, administering thyroxine will trigger metamorphosis.
Because the thyroid concentrates this element, it also concentrates the various radioactive isotopes of iodine produced by nuclear fission. In the event of large accidental releases of such material into the environment, the uptake of radioactive iodine isotopes by the thyroid can, in theory, be blocked by saturating the uptake mechanism with a large surplus of non-radioactive iodine, taken in the form of potassium iodide tablets. One consequence of the Chernobyl disaster was an increase in thyroid cancers in children in the years following the accident.[28]
The use of iodised salt is an efficient way to add iodine to the diet. It has eliminated endemic cretinism in most developed countries, and some governments have made the iodination of flour, cooking oil, and salt mandatory. Potassium iodide and sodium iodide are typically used forms of supplemental iodine.
As with most substances, either too much or too little can cause problems. Recent studies on some populations are showing that excess iodine intake could cause an increased prevalence of autoimmune thyroid disease, resulting in permanent hypothyroidism.[29]
History
There are several findings that evidence a great interest for thyroid disorders just in the Medieval Medical School of Salerno (12th century). Rogerius Salernitanus, the Salernitan surgeon and author of "Post mundi fabricam" (around 1180) was considered at that time the surgical text par excellence all over Europe. In the chapter "De bocio" of his magnum opus, he describes several pharmacological and surgical cures, some of which nowadays are reappraised quite scientifically effective.[30]
In modern times, the thyroid was first identified by the anatomist Thomas Wharton (whose name is also eponymised in Wharton's duct of the submandibular gland) in 1656.[31]
Thyroxine was identified only in the 19th century.
In 1909, Theodor Kocher from Switzerland won the Nobel Prize in Medicine "for his work on the physiology, pathology and surgery of the thyroid gland".[32]
In other animals
The thyroid gland is found in all vertebrates. In fish, it is usually located below the gills and is not always divided into distinct lobes. However, in some teleosts, patches of thyroid tissue are found elsewhere in the body, associated with the kidneys, spleen, heart, or eyes.[33]
In tetrapods, the thyroid is always found somewhere in the neck region. In most tetrapod species, there are two paired thyroid glands - that is, the right and left lobes are not joined together. However, there is only ever a single thyroid gland in most mammals, and the shape found in humans is common to many other species.[33]
In larval lampreys, the thyroid originates as an exocrine gland, secreting its hormones into the gut, and associated with the larva's filter-feeding apparatus. In the adult lamprey, the gland separates from the gut, and becomes endocrine, but this path of development may reflect the evolutionary origin of the thyroid. For instance, the closest living relatives of vertebrates, the tunicates and Amphioxus, have a structure very similar to that of larval lampreys, and this also secretes iodine-containing compounds (albeit not thyroxine).[33]
Additional images
-
 Position of the Thyroid in Males and Females
Position of the Thyroid in Males and Females -

-
 Section of the neck at about the level of the sixth cervical vertebra.
Section of the neck at about the level of the sixth cervical vertebra. -
 Muscles of the neck. Anterior view.
Muscles of the neck. Anterior view. -
 The arch of the aorta, and its branches.
The arch of the aorta, and its branches. -
 Superficial dissection of the right side of the neck, showing the carotid and subclavian arteries.
Superficial dissection of the right side of the neck, showing the carotid and subclavian arteries. -
 Diagram showing common arrangement of thyroid veins.
Diagram showing common arrangement of thyroid veins. -
 Sagittal section of nose mouth, pharynx, and larynx.
Sagittal section of nose mouth, pharynx, and larynx. -
 Muscles of the pharynx, viewed from behind, together with the associated vessels and nerves.
Muscles of the pharynx, viewed from behind, together with the associated vessels and nerves. -
 The position and relation of the esophagus in the cervical region and in the posterior mediastinum. Seen from behind.
The position and relation of the esophagus in the cervical region and in the posterior mediastinum. Seen from behind. -
 Section of thyroid gland of sheep. X 160.
Section of thyroid gland of sheep. X 160. -
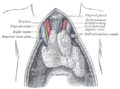 The thymus of a full-term fetus, exposed in situ.
The thymus of a full-term fetus, exposed in situ. -
 Thyoid histology
Thyoid histology -
 Thyroid
Thyroid -
 Thyroid gland
Thyroid gland -
 Thyroid gland
Thyroid gland -
 Thyroid cartilage lamina
Thyroid cartilage lamina

















See also
References
- ^ Clinical Case - Anterior Triangle of the Neck.
- ^ Yalçin B., Ozan H. (2006). "Detailed investigation of the relationship between the inferior laryngeal nerve including laryngeal branches and ligament of Berry". Journal of the American College of Surgeons. 202 (2): 291–6. doi:10.1016/j.jamcollsurg.2005.09.025. PMID 16427555.
{{cite journal}}: Unknown parameter|month=ignored (help) - ^ Lemaire, David (2005-05-27). "eMedicine - Thyroid anatomy". Retrieved 2008-01-19.
- ^ Kamath, M. Aroon. "Are the ligaments of Berry the only reason why the thyroid moves up with deglutition?". Doctors Lounge Website. Retrieved August 24, 2010.
- ^ Venturi, S; Donati, FM; Venturi, A; Venturi, M (2000). "Environmental iodine deficiency: A challenge to the evolution of terrestrial life?". Thyroid : official journal of the American Thyroid Association. 10 (8): 727–9. doi:10.1089/10507250050137851. PMID 11014322.
- ^ Küpper FC; Carpenter LJ; McFiggans GB; et al. (2008). "Iodide accumulation provides kelp with an inorganic antioxidant impacting atmospheric chemistry" (Free full text). Proceedings of the National Academy of Sciences of the United States of America. 105 (19): 6954–8. doi:10.1073/pnas.0709959105. PMC 2383960. PMID 18458346.
- ^ a b Page 493 (Table 33-3) in: Eugster, Erica A.; Pescovitz, Ora Hirsch (2004). Pediatric endocrinology: mechanisms, manifestations and management. Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 0-7817-4059-2.
{{cite book}}: CS1 maint: multiple names: authors list (link) - ^ Zoeller RT (2003). "Transplacental thyroxine and fetal brain development". J. Clin. Invest. 111 (7): 954–7. doi:10.1172/JCI18236. PMC 152596. PMID 12671044.
{{cite journal}}: Unknown parameter|month=ignored (help) - ^ Berbel P, Navarro D, Ausó E, Varea E, Rodríguez AE, Ballesta JJ, Salinas M, Flores E, Faura CC; et al. (2010). "Role of late maternal thyroid hormones in cerebral cortex development: an experimental model for human prematurity". Cereb Cortex. 20 (6): 1462–75. doi:10.1093/cercor/bhp212. PMC 2871377. PMID 19812240.
{{cite journal}}: Explicit use of et al. in:|author=(help)CS1 maint: multiple names: authors list (link) - ^ Fawcett, Don (2002). Bloom & Fawcett's Concise Histology. New York: Arnold Publishers. pp. 257–258. ISBN 0-340-80677-X.
{{cite book}}: Unknown parameter|coauthors=ignored (|author=suggested) (help) - ^ a b How Your Thyroid Works: A Delicate Feedback Mechanism. Updated 2009-05-21.
- ^ a b The thyroid gland in Endocrinology: An Integrated Approach by Stephen Nussey and Saffron Whitehead (2001) Published by BIOS Scientific Publishers Ltd. ISBN 1-85996-252-1 .
- ^ References used in image are found in image article in Commons:Commons:File:Thyroid_system.png#References.
- ^ Boron WF, Boulpaep E (2003). "Chapter 48: "synthesis of thyroid hormones"". Medical Physiology: A Cellular And Molecular Approaoch. Elsevier/Saunders. p. 1300. ISBN 1-4160-2328-3.
- ^ How Iodide Reaches its Site of Utilisation in the Thyroid Gland – Involvement of Solute Carrier 26A4 (Pendrin) and Solute Carrier 5A8 (Apical Iodide Transporter) - a report by Bernard A Rousset. Touch Brieflings 2007
- ^ Ekholm R, Bjorkman U (1997). "Glutathione peroxidase degrades intracellular hydrogen peroxide and thereby inhibits intracellular protein iodination in thyroid epithelium". Endocrinology. 138 (7): 2871–2878. doi:10.1210/en.138.7.2871. PMID 9202230.
- ^ Bianco AC, Salvatore D, Gereben B, Berry MJ, Larsen PR (2002). "Biochemistry, cellular and molecular biology, and physiological roles of the iodothyronine selenodeiodinases". Endocr Rev. 23 (1): 38–89. doi:10.1210/er.23.1.38. PMID 11844744.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ Kester MH, Martinez de Mena R, Obregon MJ, Marinkovic D, Howatson A, Visser TJ, Hume R, Morreale de Escobar G (2004). "Iodothyronine levels in the human developing brain: major regulatory roles of iodothyronine deiodinases in different areas". J Clin Endocrinol Metab. 89 (7): 3117–3128. doi:10.1210/jc.2003-031832. PMID 15240580.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ a b Jansen J, Friesema EC, Milici C, Visser TJ (2005). "Thyroid hormone transporters in health and disease". Thyroid. 15 (8): 757–68. doi:10.1089/thy.2005.15.757. PMID 16131319.
{{cite journal}}: Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ Johannes W. Dietrich (2002). Der Hypophysen-Schilddrüsen-Regelkreis. Berlin, Germany: Logos-Verlag Berlin. ISBN 978-3-89722-850-4. OCLC 50451543. 3897228505Template:Inconsistent citations
{{cite book}}: CS1 maint: postscript (link) - ^ Thyroid Problems eMedicine Health. Retrieved on 2010-02-07
- ^ Thyroid Disorders Information MedicineNet. Retrieved on 2010-02-07
- ^ Treatment for Thyroid disease Retrieved on 2010-02-07
- ^ Thyroid Disorders overview Merck Sharpe & Dohme. Retrieved on 2010-02-07
- ^ Yamamoto M, Shibuya N, Chen LC, Ogata E (1988). "Seasonal recurrence of transient hypothyroidism in a patient with autoimmune thyroiditis". Endocrinol. Jpn. 35 (1): 135–42. doi:10.1507/endocrj1954.35.135. PMID 3396511.
{{cite journal}}: Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ Hidaka Y, Amino N, Iwatani Y, Itoh E, Matsunaga M, Tamaki H (1993). "Recurrence of thyrotoxicosis after attack of allergic rhinitis in patients with Graves' disease". J. Clin. Endocrinol. Metab. 77 (6): 1667–70. doi:10.1210/jc.77.6.1667. PMID 8263157.
{{cite journal}}: Unknown parameter|month=ignored (help)CS1 maint: multiple names: authors list (link) - ^ http://www.endocrineweb.com/TFT.html
- ^ "Chernobyl children show DNA changes". BBC News. 2001-05-08. Retrieved 2010-05-25.
- ^ Patrick L (2008). "Iodine: deficiency and therapeutic considerations" (PDF). Altern Med Rev. 13 (2): 116–27. PMID 18590348.
{{cite journal}}: Unknown parameter|month=ignored (help) - ^ Bifulco M, Cavallo P (2007). "Thyroidology in the medieval medical school of salerno". Thyroid. 17 (1): 39–40. doi:10.1089/thy.2006.0277. PMID 17274747.
- ^ Thomas Wharton at Who Named It?
- ^ "The Nobel Prize in Physiology or Medicine 1909". Nobel Foundation. Retrieved 2007-07-28.
- ^ a b c Romer, Alfred Sherwood; Parsons, Thomas S. (1977). The Vertebrate Body. Philadelphia, PA: Holt-Saunders International. pp. 555–556. ISBN 0-03-910284-X.
{kind=link}
External links
- EndocrineWeb.com for more information on thyroid disease, hormones, and surgery
- American Thyroid Association (Thyroid Information and professional organization)
- Histology at KUMC epithel-epith03 "Thyroid Gland"
Anatomy and morphology | ||
|---|---|---|
| Fields |  | |
| Bacteria and fungi | ||
| Protists | ||
| Plants | ||
| Invertebrates | ||
| Mammals | ||
| Other vertebrates | ||
| Glossaries | ||
| Related topics | ||