
Talk:COVID-19 pandemic in the United States: Difference between revisions
Dan Polansky (talk | contribs) |
→IHME projections for the U.S.: comment |
||
| Line 361: | Line 361: | ||
:::: On another note, I was once more reverted using "reverted third removal in a day by same editor [...]", which is inaccurate: I only removed the material two times on this day, each time with a different rationale; the last reversion of my removal is weak on process and completely silent on substance. --[[User:Dan Polansky|Dan Polansky]] ([[User talk:Dan Polansky|talk]]) 14:09, 7 September 2020 (UTC) |
:::: On another note, I was once more reverted using "reverted third removal in a day by same editor [...]", which is inaccurate: I only removed the material two times on this day, each time with a different rationale; the last reversion of my removal is weak on process and completely silent on substance. --[[User:Dan Polansky|Dan Polansky]] ([[User talk:Dan Polansky|talk]]) 14:09, 7 September 2020 (UTC) |
||
:::: On ''efficacy'': The article says "The Institute for Health Metrics and Evaluation (IHME) predicted that universal wearing of face masks could prevent 17,000–28,000 deaths between June 26 and October 1, 2020"; that is a clear efficacy claim, a claim that mask weaking saves so and so many lives. It traces to material that is not peer-reviewed science. --[[User:Dan Polansky|Dan Polansky]] ([[User talk:Dan Polansky|talk]]) 14:12, 7 September 2020 (UTC) |
:::: On ''efficacy'': The article says "The Institute for Health Metrics and Evaluation (IHME) predicted that universal wearing of face masks could prevent 17,000–28,000 deaths between June 26 and October 1, 2020"; that is a clear efficacy claim, a claim that mask weaking saves so and so many lives. It traces to material that is not peer-reviewed science. --[[User:Dan Polansky|Dan Polansky]] ([[User talk:Dan Polansky|talk]]) 14:12, 7 September 2020 (UTC) |
||
:::::Mainstream sources are generally reliable, and certainly usable for statistical modeling properly attributed to IHME. I disagree that there is a medical efficacy claim at play. - [[user:MrX|MrX]][[user talk:MrX| 🖋]] 14:46, 7 September 2020 (UTC) |
|||
== Semi-protected edit request on 6 September 2020 == |
== Semi-protected edit request on 6 September 2020 == |
||
Revision as of 14:46, 7 September 2020
Daily pageviews of this article
A graph should have been displayed here but graphs are temporarily disabled. Until they are enabled again, visit the interactive graph at pageviews.wmcloud.org |
| This is the talk page for discussing improvements to the COVID-19 pandemic in the United States article. This is not a forum for general discussion of the article's subject. |
Article policies
|
| Find medical sources: Source guidelines · PubMed · Cochrane · DOAJ · Gale · OpenMD · ScienceDirect · Springer · Trip · Wiley · TWL |
| Archives: Index, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17Auto-archiving period: 10 days |
| The contentious topics procedure applies to this page. This page is related to post-1992 politics of the United States and closely related people, which has been designated as a contentious topic. Editors who repeatedly or seriously fail to adhere to the purpose of Wikipedia, any expected standards of behaviour, or any normal editorial process may be blocked or restricted by an administrator. Editors are advised to familiarise themselves with the contentious topics procedures before editing this page. |
WikiProject COVID-19 consensus WikiProject COVID-19 aims to add to and build consensus for pages relating to COVID-19. They have so far discussed items listed below. Please discuss proposed improvements to them at the project talk page.
To ensure you are viewing the current list, you may wish to . |
| This article is of interest to multiple WikiProjects. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
.svg)





| This article is written in American English, which has its own spelling conventions (color, defense, traveled) and some terms that are used in it may be different or absent from other varieties of English. According to the relevant style guide, this should not be changed without broad consensus. |
| This is the talk page for discussing improvements to the COVID-19 pandemic in the United States article. This is not a forum for general discussion of the article's subject. |
Article policies
|
| Find medical sources: Source guidelines · PubMed · Cochrane · DOAJ · Gale · OpenMD · ScienceDirect · Springer · Trip · Wiley · TWL |
| Archives: Index, 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17Auto-archiving period: 10 days |
|
 | The following references may be useful when improving this article in the future:
|
Mortality in the United States
The lead ought to say that the total number of deaths in the U.S. is the world's highest. My source is Johns Hopkins Cases and mortality by country. Why doesn't the first paragraph state this very basic fact? -SusanLesch (talk) 17:18, 20 August 2020 (UTC)
- The fact should be excluded since it is irrelevant: it above all reflects on how populous a country is. It would be hard for a small country to lead by the number of deaths no matter how bad its covid handling. The discussed statement is true, but irrelevant and arguably misleading. Instead of the absolute number, the article relevantly states the relative number AKA death rate: "As of August 20, its death rate had reached 529 per million people, the eleventh-highest rate globally." --Dan Polansky (talk) 09:32, 21 August 2020 (UTC)
Specific outbreaks, plagues, and epidemics in the United States lists a number of epidemics and most of them carry a fatality number in the first paragraph. List of epidemics offers only the total number who died. Hardly irrelevant. I'm tired of arguing with you. -SusanLesch (talk) 19:47, 21 August 2020 (UTC)
- If you're talking blame, then such a number would be weird to mention maybe. However, if you're talking about the impact that the pandemic has had on a country, it seems fair to also point out that the number is highest in absolute sense. For balance sake, you may want to point out as well how that compares to a typical impact on other countries (e.g. mortality). effeietsanders 21:49, 21 August 2020 (UTC)
- PS: @Susan: the way I read it, Dan is not really against mentioning the number, but rather whether that is the 'highest' country in the world.
- Right. For a comparison between countries, the absolute death count is meaningless. And "the world's highest" is a comparison between countries. As for mentioning the absolute death count, it is in the infobox, and I do not propose to remove it from there. --Dan Polansky (talk) 12:14, 23 August 2020 (UTC)
- The impact of a pandemic on a country really does not depend directly on the absolute count; it depends on the relative count, that is, deaths per million pop. Similar for unemployment: the absolute count of unemployed people does not directly reveal the severity of unemployment; it is the percent of people unemployed that indicates the severity. --Dan Polansky (talk) 12:22, 23 August 2020 (UTC)
- Per all the examples in Wikipedia's list of epidemics I added a total to the lead paragraph. That number is important when we compare epidemic to epidemic. -SusanLesch (talk) 17:01, 23 August 2020 (UTC)
- I removed the sentence in diff: the number is in the infobox and the indicated relation to the world's count is likely to be misleading. The non-misleading death per million is already in the article. Unlike the present article, list of epidemics does not give epidemics per country, and therefore, inter-county comparison does not become a problem in articles it links to. --Dan Polansky (talk) 20:24, 23 August 2020 (UTC)
- I would request to revert that - the phrase was quite neutral, and I disagree it is meaningless. We should not rely on infoboxes to confer essential information. The fact that about 20% of the worldwide deaths are in the US, is a meaningful piece of information in an article about the pandemic in the US. I would agree that this is misleading in an article about the pandemic in general - but if you're describing the US, it helps to provide some context of how it relates to the worldwide pandemic. effeietsanders 20:57, 23 August 2020 (UTC)
- What I removed is this: "As of August 2020, 170,000 of the world's 800,000 deaths from COVID-19 occurred in the U.S." The comparison to world's absolute death count is not neutral; it artificially makes U.S. look worse than it is. This becomes obvious when one uses the same sentence form for e.g. Belgium: "9,872 of the world's 800,000 deaths from COVID-19 occurred in Belgium." In this sentence, Belgium does not look bad yet it has more deaths per capita than U.S., and that is the true indicator of severity. The sentence removed by me is another attempt to sneak in invalid inter-country comparison of absolute numbers. --Dan Polansky (talk) 08:08, 27 August 2020 (UTC)
- I think you're over interpreting language. This is not what I would read into that at all - it states clearly that the US is heavily impacted, but also clearly signals that it is not just the United States. An example of why it can be confusing in a different context: in the article Ebola virus epidemic in Liberia does mention how many people died, but it does not mention anything about the worldwide impact of the virus. This means we lack context that the 4800 deaths was almost half the worldwide death count, showing that this was an epicenter of the disease.
- It feels like you're reading some kind of judgement into the sentence, while it is mostly providing context on the worldwide stage. effeietsanders 01:51, 28 August 2020 (UTC)
- I explained above the comparison to be misleading, but apparently to deaf ears. In any case, you noticed the comparison is not made in Ebola virus epidemic in Liberia; do you know of a single Wikipedia article making that comparison? Let us notice that the comparison was inserted by someone who said "The lead ought to say that the total number of deaths in the U.S. is the world's highest", proposing to add sophistry to the lead; that same person seems to think that the PIRG letter is more than a low-grade timewaster. We shall be neutral. --Dan Polansky (talk) 12:06, 30 August 2020 (UTC)
- What I removed is this: "As of August 2020, 170,000 of the world's 800,000 deaths from COVID-19 occurred in the U.S." The comparison to world's absolute death count is not neutral; it artificially makes U.S. look worse than it is. This becomes obvious when one uses the same sentence form for e.g. Belgium: "9,872 of the world's 800,000 deaths from COVID-19 occurred in Belgium." In this sentence, Belgium does not look bad yet it has more deaths per capita than U.S., and that is the true indicator of severity. The sentence removed by me is another attempt to sneak in invalid inter-country comparison of absolute numbers. --Dan Polansky (talk) 08:08, 27 August 2020 (UTC)
- I would request to revert that - the phrase was quite neutral, and I disagree it is meaningless. We should not rely on infoboxes to confer essential information. The fact that about 20% of the worldwide deaths are in the US, is a meaningful piece of information in an article about the pandemic in the US. I would agree that this is misleading in an article about the pandemic in general - but if you're describing the US, it helps to provide some context of how it relates to the worldwide pandemic. effeietsanders 20:57, 23 August 2020 (UTC)
- I removed the sentence in diff: the number is in the infobox and the indicated relation to the world's count is likely to be misleading. The non-misleading death per million is already in the article. Unlike the present article, list of epidemics does not give epidemics per country, and therefore, inter-county comparison does not become a problem in articles it links to. --Dan Polansky (talk) 20:24, 23 August 2020 (UTC)
- Per all the examples in Wikipedia's list of epidemics I added a total to the lead paragraph. That number is important when we compare epidemic to epidemic. -SusanLesch (talk) 17:01, 23 August 2020 (UTC)
This article needs to say to readers that the number of deaths in the U.S. is the highest in the world. That is, the death toll, or absolute number of total deaths, simply, the actual number of people who died here in context. It is true per the best source we have, Johns Hopkins University. It is not sneaky or sophistry, invalid or dubious or irrelevant; those are your words and interpretations. -SusanLesch (talk) 16:41, 30 August 2020 (UTC)
- @Dan: I'm not sure if this ad hominem is very helpful. I have heard your argument about neutral, I just don't agree that your removal of this context is actually making the article more neutral; au contraire. My impression is that your attitude towards removing data that feels too painful to mention, may result in downplaying the impact of this pandemic on the United States - which by itself is again not unbiased. effeietsanders 20:55, 31 August 2020 (UTC)
- To avoid repetition of what I already said above, I will referain from raising obvious objections to some points above. The reader is well advised to consult e.g. File:COVID-19 Outbreak World Map Total Deaths per Capita.svg to see how the death rate in the U.S. compares to other countries, and get a relevant picture rather than partisan invalid comparison of absolute numbers between countries. It would be also of interest to have a chart or table of excess death per capita for various countries, but I do not know of any source providing such a table.
- Outstanding unanswered question: you (Effeietsanders) noticed the comparison is not made in Ebola virus epidemic in Liberia; do you know of a single Wikipedia article making that comparison? That is, do you know of a single Wikipedia article that is on an epidemic in a particular country and compares the absolute deaths in that country with worldwide deaths? Or do you know of a peer-reviewed scientific article making such a comparison? --Dan Polansky (talk) 09:58, 2 September 2020 (UTC)
- Why don't you address any of the specific arguments I made above? You just repeated the same assertion without any proof or further articulation. Why don't you for instance address this: "it [the absolute death count] above all reflects on how populous a country is". --Dan Polansky (talk) 14:56, 2 September 2020 (UTC)
- Dan Polansky, addressing your point: if your measure is true, "[the absolute death count] above all reflects on how populous a country is", then the US must have 21.5% of the world's population. -SusanLesch (talk) 18:02, 2 September 2020 (UTC)
- It's above all, not solely. The death count depends on 1) death rate (the relevant measure), and 2) population. We already report 1) and use it for inter-country comparison; 2) just adds confusion to the measure. The U.S. death rate is on the similar order as many other countries (500-1000 per million pop), and that is the relevant comparison. Put differently, as for death rate, the U.S. is in the same first league as many other countries, and which country has which exact rank in that league is of no scientific significance. Of note is that we have no reliable data from the very populous China; they don't even tell us how many tests they are doing. --Dan Polansky (talk) 09:01, 3 September 2020 (UTC)
- Dan Polansky, and others. Your editing of the following RFC is welcome before I post it about 24 hours from now. Two weeks is too long to argue and we don't appear to be getting anywhere. -SusanLesch (talk) 14:12, 3 September 2020 (UTC)
- It's above all, not solely. The death count depends on 1) death rate (the relevant measure), and 2) population. We already report 1) and use it for inter-country comparison; 2) just adds confusion to the measure. The U.S. death rate is on the similar order as many other countries (500-1000 per million pop), and that is the relevant comparison. Put differently, as for death rate, the U.S. is in the same first league as many other countries, and which country has which exact rank in that league is of no scientific significance. Of note is that we have no reliable data from the very populous China; they don't even tell us how many tests they are doing. --Dan Polansky (talk) 09:01, 3 September 2020 (UTC)
- Dan Polansky, addressing your point: if your measure is true, "[the absolute death count] above all reflects on how populous a country is", then the US must have 21.5% of the world's population. -SusanLesch (talk) 18:02, 2 September 2020 (UTC)
{kind=link}
Proposed RFC
- Should the lead inform the reader that the United States has more than 20% of the world's mortality from COVID-19?
- One view prefers deaths per capita as a measure of severity.
- The other view is that the context of the US fraction is important for understanding.
- Yes or No. Previous discussion. ::::-SusanLesch (talk) 14:12, 3 September 2020 (UTC)
- Should the lead inform the reader that the United States has more than 20% of the world's mortality from COVID-19?
- No. I agree with what Dan Polansky wrote at 12:14 on 23 August 2020 (UTC): "For a comparison between countries, the absolute death count is meaningless. And 'the world's highest' is a comparison between countries." Mark D Worthen PsyD (talk) [he/his/him] 20:11, 4 September 2020 (UTC)
- Comment Please share your opinions at #RFC on mortality. 2601:5C6:8081:35C0:1C4:1766:5D51:7D23 (talk) 23:51, 6 September 2020 (UTC)
Too many graphs/charts
I stopped by this article for the first time in quite a while today, and I see it currently exceeds the PEIS limit, and also has a ton of charts and graphs. Those are presumably related, so my advice for any of you trying to figure out how to get it back under the limit would be to drop the unneeded ones. As to which ones should go, I'll leave that to those of you who have been following this page more closely. {{u|Sdkb}} talk 08:05, 26 August 2020 (UTC)
- Most of the charts are useful and non-rendundant. To address the PEIS problem, one should investigate the actual largest contributor to the problem. For a start, the transcluded Template:COVID-19 pandemic data/United States medical cases by state shows abundant low-value-added use of templates.
- The Template:COVID-19 pandemic data/United States medical cases by state provides a very good quick overview of the state of affairs in various parts of the country in a quick readable format. It's more difficult to read historical data points and keep scrolling to the bottom in tables where cases are listed by dates. The the other tables are more difficult to read in a script for researchers as well. --GoodOldSam (talk) 19:54, 3 September 2020 (UTC)
- Should some charts be removed, I would see the three charts in Number of U.S. cases by date section as the foremost candidates: they contain a line for each state (50 lines in total?) and thus are quite large in terms of wikitext (about 39 KB), and yet the value they provide seems rather limited. By contrast, all the charts in Progression charts section have about 57 KB, yet provide much more valuable picture. (For reference: Wikipedia:PEIS.)
- To help a little, I went ahead and reduced the data amount in one of the charts I have added: diff. --Dan Polansky (talk) 09:04, 27 August 2020 (UTC)
- The all-cause death graphs are the least important; I'm sure various causes of deaths are affected to different degrees (deaths from flu(non-covid-19), car accidents, roller coaster accidents, etc) so pooling across causes despite the interaction with the pandemic isn't very appropriate. Also the deaths by year isn't adjusted by population, or population age, so it's hard to see the interaction, but the graphs above already make the case that deaths have increased this year. Of 19 (talk) 04:56, 29 August 2020 (UTC)
- To the contrary, I find the all-cause death graphs to be very important, showing the covid in proportion to baseline deaths and showing that covid deaths are very likely more than just misattributed deaths for other causes. As for "so pooling across causes despite the interaction with the pandemic isn't very appropriate", that makes no sense to me at all. My words seem confirmed by the introductory paragraph of mortality.org[1]: "In response to the COVID-19 pandemic, the HMD team decided to establish a new data resource: Short-term Mortality Fluctuations (STMF) data series. Objective and internationally comparable data are crucial to determine the effectiveness of different strategies used to address epidemics. Weekly death counts provide the most objective and comparable way of assessing the scale of short-term mortality elevations across countries and time." --Dan Polansky (talk) 11:54, 30 August 2020 (UTC)
- The all-cause death graphs are the least important; I'm sure various causes of deaths are affected to different degrees (deaths from flu(non-covid-19), car accidents, roller coaster accidents, etc) so pooling across causes despite the interaction with the pandemic isn't very appropriate. Also the deaths by year isn't adjusted by population, or population age, so it's hard to see the interaction, but the graphs above already make the case that deaths have increased this year. Of 19 (talk) 04:56, 29 August 2020 (UTC)
Dropping semilog-chart with cases and deaths but not tests

I am again about to drop a semilog-chart with cases and deaths but not tests. It is misleading in that its straigt-line portions suggest there was exponential growth but since tests are not plotted, it is not obvious that the apparent exponential growth had to do with exponential growth of tests. The chart even suggests exponential growth by adding straight trend lines. We must not mislead. --Dan Polansky (talk) 09:16, 27 August 2020 (UTC)
- I'm not sure, but just checking: are you arguing that the increase in cases and deaths is primarily because of the increase in tests? I'm not sure if I'm reading this right.
- I think these charts are very insightful for the first period of time. Maybe they should simply be cut off at a certain point. I suggest you create an alternative version that you find more helpful, rather than dropping stuff. Adding number of tests is helpful information if there are rapid changes in the number of tests - but the trends are more comparing one day to the next, and it seems fair to assume that these days see roughly the same number of tests. effeietsanders 01:44, 28 August 2020 (UTC)
- I am saying that the initial exponential increase of confirmed cases was due to initial exponential increase of tests; this is confirmed in the test positivity rate chart. The word "exponential" in my statements is important and is absent from "increase in cases and deaths is primarily because of the increase in tests"; there is no doubt that even under constant daily test regime, there will be new daily confirmed cases and new covid-coded deaths for some time to come. Again, the word exponential is key. --Dan Polansky (talk) 11:49, 30 August 2020 (UTC)
- Moreover, the discussed chart is largely redundant to the third chart in COVID-19 pandemic in the United States#Progression charts, with the difference that the chart we include does not show any exponential trendlines. Using the argument I made, also the chart currently included is problematic but at least it does not suggest any trendlines; tests can be added to the currently included chart. --Dan Polansky (talk) 14:11, 30 August 2020 (UTC)
Death rate trend since July - calculations
I did some mathematical work on US Covid-19 deaths in mid-July, reported and discussed here but since archived. I simply took the figures from this article for 1-15 July and did a least-squares exponential fit; the result was y = 116.7645323 exp(5.178324329 × 10^-3 x), where x is day number, 1 for 1 July, etc., and y is number of deaths. This is a totally mindless mathematical fit with no modelling or assumptions, no selection of data, using, as I said the data from the article - anyone can repeat this. I extrapolated the figures beyond this period; I posted some extrapolated numbers here (now archived), saying very clearly that this was not a prediction. In fact, as I said, I expected that the real numbers would be lower than the extrapolation as measures to control the epidemic kicked in.
I have not done any further work, I'm still using the extrapolation from 1-15 July. The extrapolated figure for 1 September (day 63 from 1 July) is 161,805. The actual number of deaths as reported in the article under the heading "COVID-19 cases in the United States" is 172,978, which I found a shock. It indicates that growth since the first half of July is significantly greater than the exponential growth in that period.
It is very easy to replicate these calculations using data from the article, and also to use a different base period for the extrapolation - there is zero input from me, zero selection, zero knowledge, zero skill (except the ability to do a least-squares exponential fit). Possibly this information will be useful for those working on the article (I haven't made any significant edits beyond improving wording).
Best wishes, Pol098 (talk) 19:41, 2 September 2020 (UTC)
- There is nothing above to be taken seriously. I commented on the above in Talk:COVID-19_pandemic_in_the_United_States/Archive_13#Exponential fit. There was nothing meaningful in the fitting. The exponential business is nonsense. Current U.S. new daily deaths, 7-day average, are slowly declining, excellent news; the recent peak was about 1200 new deaths per day and it has now declined to under 900 new deaths per day[2]. Current hospitalizations have been declining for over 30 days[3], and are down from recent peak of 60,000 to today's 35,600. For the lay reader, there is currently no exponential growth of total deaths since if that were so, there would be exponential growth of daily new deaths, which are declining instead. --Dan Polansky (talk) 09:16, 3 September 2020 (UTC)
- If the reader cannot resist the temptation to look at death projections, I can recommend Talk:COVID-19 pandemic in the United States/Archive 14#Simplistic death projection, which includes my very simplistic projections and also projections by nobel laureate Michael Levitt. --Dan Polansky (talk) 09:34, 3 September 2020 (UTC)
- I generally agree with Dan Polansky; mine was a purely mathematical exercise, and I expected it to be overly pessimistic. The one comment I disagree with, if taken literally, is "The exponential business is nonsense". While, indeed, it isn't a prediction and shouldn't be taken as such, the exponential fit for the limited period in which I applied it is very good, surprisingly so, it is the appropriate simple function to fit the figures. There is a graph that is sometimes added to the article, deleted when it goes out of date, and re-added when it is updated (currently not included) which shows the figures to be visually very close to a straight line for extended periods if plotted on a logarithmic scale, i.e., the curve is exponential. So, the exponential nature of the growth is not necessarily significant or predictive, but it is a fact of the past progression. Best wishes, Pol098 (talk) 10:49, 3 September 2020 (UTC)
- The exponential business really is nonsense; as per #Dropping semilog-chart with cases and deaths but not tests above, the initial exponential increase of confirmed cases was due to initial exponential increase of tests, and a similar consideration holds true for initial growth of covid-coded deaths. The daily new deaths have been in decline since Aug 1, and therefore, the total death curve has not been exponential at least since Aug 1, over 30 days. That is a very obvious consideration. --Dan Polansky (talk) 11:14, 3 September 2020 (UTC)
- I generally agree with Dan Polansky; mine was a purely mathematical exercise, and I expected it to be overly pessimistic. The one comment I disagree with, if taken literally, is "The exponential business is nonsense". While, indeed, it isn't a prediction and shouldn't be taken as such, the exponential fit for the limited period in which I applied it is very good, surprisingly so, it is the appropriate simple function to fit the figures. There is a graph that is sometimes added to the article, deleted when it goes out of date, and re-added when it is updated (currently not included) which shows the figures to be visually very close to a straight line for extended periods if plotted on a logarithmic scale, i.e., the curve is exponential. So, the exponential nature of the growth is not necessarily significant or predictive, but it is a fact of the past progression. Best wishes, Pol098 (talk) 10:49, 3 September 2020 (UTC)
Let me plot the total deaths on a normal scale:
| Graphs are unavailable due to technical issues. There is more info on Phabricator and on MediaWiki.org. |
--Dan Polansky (talk) 11:23, 3 September 2020 (UTC)
Let me plot another chart, one that shows for each date the ratio of its total death value to the value of the previous date, of that 7-day moving average. That is, the chart shows what the base for exponential growth would be if it really were exponential growth:
| Graphs are unavailable due to technical issues. There is more info on Phabricator and on MediaWiki.org. |
--Dan Polansky (talk) 11:46, 3 September 2020 (UTC)
And let me show only part of the chart so that the low values are more distinct:
| Graphs are unavailable due to technical issues. There is more info on Phabricator and on MediaWiki.org. |
--Dan Polansky (talk) 11:55, 3 September 2020 (UTC)
- Just for the hell of it I've done another mindless mathematical exercise, which I do not claim reflects reality at all (just that it's mathematically accurate). Looking at the last of the 3 graphs of Dan Polansky, I eyeball a rate of increase of very roughly 0.5% deaths per day (assuming that the graph approximates to a horizontal straight line for the last few weeks). I have made just one mathematical calculation, with no selection or tuning, I just plugged in a daily increase of 0.5% from the extrapolated figure of 163490 (lower than the actual reported number) for today, 3 Sep 20, and ran it to 17 Nov 20, which is where I ended the exponential fit. I find the exponential fit (extended from the first 15 days of July) extrapolates to 241,079; a 0.5%/day increase from 4 Sep gives 241,033 for the same date, which I find astonishingly close to the exponential, particularly as I just eyeballed the 0.5% figure. The fit is close for every day, 17 Nov is not "privileged" or specially selected. Making a brief foray into reality, the %/day curve does seem to be trending down since the beginning of August (steadily reducing from 0.8% to 0.55%), so hopefully the numbers produced by the mindless mathematics are pessimistic. And obviously any major medical development will change things radically. Pol098 (talk) 13:14, 3 September 2020 (UTC)
- And yet the total death curve was growing less than linearly for the whole of August, let alone exponentially. I don't understand the above mindset. This whole talk of "exponential growth" used for modelling this epidemic is a dangerous nonsense, one that I have fallen for myself initially. (I hate to admit as much.) --Dan Polansky (talk) 13:57, 3 September 2020 (UTC)
Recently Removed State Cases Table
First of all, thanks to everyone who contributes to this page, and especially to the person who periodically updated what I believe was titled the State Cases Table. To clarify if I got the name of the table wrong, it contained the following columns (U.S. state or territory, Cases, Deaths, Recov., Hosp.). Over the past five months I used the data from this table to study the slow but steady growth in the number of COVID-19 deaths from the 10 states with the lowest number of deaths. I am sorry to see that support for the table was dropped. Could whoever supported that table possibly point me to the source for that table? Thank you. Bobanello (talk) 20:55, 3 September 2020 (UTC) Bobanello
- Fixed in diff. --Dan Polansky (talk) 05:54, 4 September 2020 (UTC)
Demographics pie chart
I am considering to switch the demographics bar chart to pie chart. I have the following:
COVID-19-related deaths by age group:
| Graphs are unavailable due to technical issues. There is more info on Phabricator and on MediaWiki.org. |
One thing I don't like is that the x-values are not shown in the chart, only in the legend. Does anyone know how to add the x-value lables directly to the chart?
Also, the values are shown oddly for the small portions; they should ideally not be shown at all for the small portions and only be shown for portions that are large enough to comfortably host the y-value text. --Dan Polansky (talk) 13:20, 4 September 2020 (UTC)
- I'm confused. Earlier, you make the argument that it is silly to show absolute numbers for the US without normalizing it per capita - but wouldn't the same argument apply even more strongly here? It is hard to interpret these numbers without providing context of how big these age groups are to begin with. For the US population, most people at least know it's about 300M, and the world population is about 6B. I would have a harder time guessing the percentage of people 15-24 years old.
- Aside from that, the buckets seem somewhat artificial and overly granular for young age. effeietsanders 02:32, 5 September 2020 (UTC)
- That's a good point: the absolute death counts per age group are not adjusted for age group population size. However, that would mean that the portion of the old-age people would be even larger when adjusted for age group population size. That said, the distortion is not so huge as in intercountry comparisons of death counts. I'll think about it. --Dan Polansky (talk) 06:12, 5 September 2020 (UTC)
RFC on mortality
|
Should the lead inform the reader that the United States has more than 20% of the world's mortality from COVID-19?
- One view prefers deaths per capita as a measure of severity.
- The other view is that the context of the US fraction is important for understanding.
Yes or No. Previous discussion. -16:40, 4 September 2020 (UTC)
Poll
Yes. According to Dan Polansky: "the true indicator of severity" is "deaths per capita". So I looked up reliable sources. Last semester I got an A in epidemiology but it did not prepare me to sort through these options.
- The U.S. Pandemic Severity Assessment Framework (2017) uses 7 indicators of transmissibility plus 3 main but a total of 8 severity indicators in its clinical dimension: case fatality rate, case-hospitalization ratio, deaths-hospitalization ratio, a few more, and excess deaths.
- Wu et al. in Nature sort of agrees: "The clinical severity of infectious diseases is typically measured in terms of infection fatality risk (IFR), symptomatic case fatality risk (sCFR) and hospitalization fatality risk (HFR)."
- The World Health Organization (WHO) says: "The true severity of a disease can be described by the Infection Fatality Ratio."
Wikipedia should be written for the widest possible general audience per WP:TECHNICAL, specifically WP:ONEDOWN and the guide WP:AUDIENCE. The Hemingway app says this article is post graduate level. I suggest that people who wish to do so put their thoughts into Statistics of the COVID-19 pandemic in the United States, like Statistics of COVID-19 pandemic in India and Statistics of the COVID-19 pandemic in Poland. -SusanLesch (talk) 22:11, 4 September 2020 (UTC)
- Could you phrase the proposal in a more complete sentence? This clearly stands or falls with formulation. effeietsanders 05:37, 5 September 2020 (UTC)
- Surely, I am happy to try. Should the lead state the number of deaths in the US given as a proportion of the number of deaths worldwide? The US population is about 4% of the world. Should we say here that the US death toll is about 20% of the world death toll from COVID-19? Corrections welcome. -SusanLesch (talk) 15:35, 5 September 2020 (UTC)
- The question of the poll is clearly stated: "Should the lead inform the reader that the United States has more than 20% of the world's mortality from COVID-19?" Should it or should it not? --Dan Polansky (talk) 16:01, 5 September 2020 (UTC)
- Surely, I am happy to try. Should the lead state the number of deaths in the US given as a proportion of the number of deaths worldwide? The US population is about 4% of the world. Should we say here that the US death toll is about 20% of the world death toll from COVID-19? Corrections welcome. -SusanLesch (talk) 15:35, 5 September 2020 (UTC)
- Stringing together sentences not supporting the proposal as is done above does not do the matter much good. Sure, for comparing one epidemic to another, IFR is a prime candidate for severity indicator. But for intercountry comparisons, death rate per million is fine and we do not know IFR on country level. Certainly none of the above sources indicate that absolute death count is the meaningful severity indicator. On another note, excess deaths mentioned above would also be meaningful but only when adjusted for population size, so again excess death rate per million. ("Last semester I got an A in epidemiology": I wonder what SusanLesch is studying and what the qualifications and degrees are, if we are to play this game. Maybe better stick with discussing the substance.) --Dan Polansky (talk) 06:48, 5 September 2020 (UTC)
- No. Mark D Worthen PsyD (talk) [he/his/him] 14:46, 5 September 2020 (UTC)
- No. Real figures for the world will probably never be known, per article. For instance, in April China revised its case totals much higher and increased its death toll estimate by 50%. --Light show (talk) 17:37, 5 September 2020 (UTC)
- Note that due to "both funeral urns distribution and continuous full capacity operation of cremation services," some sources estimated 10 times China's official death toll by the end of March, per a Yale preprint. --Light show (talk) 19:59, 5 September 2020 (UTC)
News agencies
Dan Polansky: I object to your edit summary, "...sources to Reuterns: we already know the numbers without Reuters and the rest is their biased story telling as part of mainstream media living from producing bad news". What possible good can come from badmouthing Reuters? -SusanLesch (talk) 18:47, 4 September 2020 (UTC)
- I see no arguments, evidence, or analysis above, and therefore there is nothing to respond to with substance. --Dan Polansky (talk) 06:36, 5 September 2020 (UTC)
- All right. That's one way to answer a question. -SusanLesch (talk) 18:53, 5 September 2020 (UTC)
- I thought it was a rhetorical question. Let me articulate the obvious, then. Mainstream media are unreliable and non-neutral; by refusing to uncritically take over problematic sentences from mainstream media, we make the encyclopedia more reliable and neutral. Reuters is part of mainstream media. The Reuters article[4] mentions IHME without at the same time indicating that IHME is unreliable: "The Institute for Health Metrics and Evaluation is anticipating an uptick in COVID-19 cases in the coming months, resulting in around 300,000 total deaths by December, and a nearly 75% increase in hospitalizations." They are doing no serious journalism, just parotting unreliable sources without critical assessment of the sources. If they wanted to quote IHME, they should have included reservations about IHME in the same paragraph; they did not. Fail. --Dan Polansky (talk) 06:40, 6 September 2020 (UTC)
- It is unreasonable to expect a global news agency to produce news at the level of detail you seem to require. I suggest you read news agency which says "All four began with and continue to operate on a basic philosophy of providing a single objective news feed to all subscribers; they do not provide separate feeds for conservative or liberal newspapers." Don't you realize we are very lucky to have them? Next time your city has an earthquake or an election what other dependable source do you plan to consult? I take offense because the business model for most of journalism has been threatened by the web and I don't enjoy it when some guy like you decides to denigrate the entire field. The other three fourths of your answer is your assertion that IHME is unreliable which is your opinion and is not a proven fact. -SusanLesch (talk) 16:34, 6 September 2020 (UTC)
- It is not unreasonable at all; it is their fulltime job, and it is very easy to do a background check on IHME. --Dan Polansky (talk) 12:07, 7 September 2020 (UTC)
- It is unreasonable to expect a global news agency to produce news at the level of detail you seem to require. I suggest you read news agency which says "All four began with and continue to operate on a basic philosophy of providing a single objective news feed to all subscribers; they do not provide separate feeds for conservative or liberal newspapers." Don't you realize we are very lucky to have them? Next time your city has an earthquake or an election what other dependable source do you plan to consult? I take offense because the business model for most of journalism has been threatened by the web and I don't enjoy it when some guy like you decides to denigrate the entire field. The other three fourths of your answer is your assertion that IHME is unreliable which is your opinion and is not a proven fact. -SusanLesch (talk) 16:34, 6 September 2020 (UTC)
- I thought it was a rhetorical question. Let me articulate the obvious, then. Mainstream media are unreliable and non-neutral; by refusing to uncritically take over problematic sentences from mainstream media, we make the encyclopedia more reliable and neutral. Reuters is part of mainstream media. The Reuters article[4] mentions IHME without at the same time indicating that IHME is unreliable: "The Institute for Health Metrics and Evaluation is anticipating an uptick in COVID-19 cases in the coming months, resulting in around 300,000 total deaths by December, and a nearly 75% increase in hospitalizations." They are doing no serious journalism, just parotting unreliable sources without critical assessment of the sources. If they wanted to quote IHME, they should have included reservations about IHME in the same paragraph; they did not. Fail. --Dan Polansky (talk) 06:40, 6 September 2020 (UTC)
- All right. That's one way to answer a question. -SusanLesch (talk) 18:53, 5 September 2020 (UTC)
"Trumpvirus" listed at Redirects for discussion
![]() A discussion is taking place to address the redirect Trumpvirus. The discussion will occur at Wikipedia:Redirects for discussion/Log/2020 September 5#Trumpvirus until a consensus is reached, and readers of this page are welcome to contribute to the discussion. –Deacon Vorbis (carbon • videos) 13:36, 5 September 2020 (UTC)
A discussion is taking place to address the redirect Trumpvirus. The discussion will occur at Wikipedia:Redirects for discussion/Log/2020 September 5#Trumpvirus until a consensus is reached, and readers of this page are welcome to contribute to the discussion. –Deacon Vorbis (carbon • videos) 13:36, 5 September 2020 (UTC)
IHME projections for the U.S.
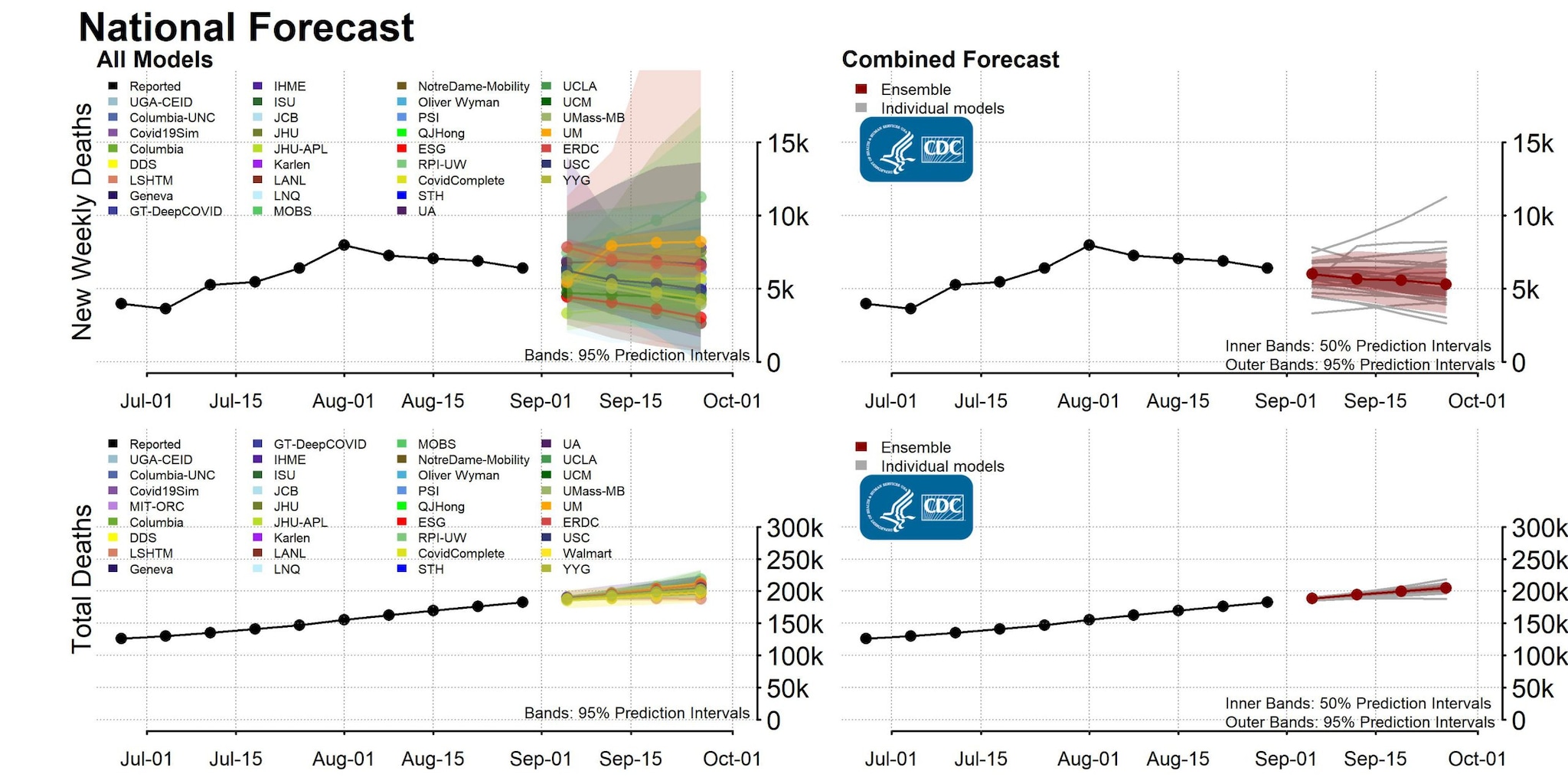
There is the following, already in the article:
Of remarkable interest in the above pdf is Fig 14, which shows multiple forecasts. In my inexpert view, the Continued SD mandate easing forecast is very inlikely and has nothing to do with science; it projects daily new confirmed cases would reach 1,000,000 per day in December. Yes, a million.
For calibration of IMHE model performance, it would be worthwhile to collect pdfs for their previous projections; if anyone knows the pdfs, please post.
A more recent pdf of a "briefing" containing similar content as the above is this:
- http://www.healthdata.org/sites/default/files/files/Projects/COVID/briefing_US_09.03.2020.pdf
- "If a herd immunity strategy is pursued, namely no further government intervention is taken from now to January 1, then the death toll could increase to 620,000 by January 1."
- Comment: What does "could" mean above? Could in the parallel universe? Could but does not have to? The sentence means close to nothing, as far as I can tell: It is not exposed to refutation even if a herd immunity strategy is pursued, since the consequent is still guarded by "could" rather than using the reasonably bold "will", "is predicted to" or "is projected to".
--Dan Polansky (talk) 15:57, 5 September 2020 (UTC)
- I'm not sure that "daily COVID-19 infections" is the same as "new confirmed cases". Whatever it represents, the prediction for several months from now is less about the big round number and more about the possibility that the number of sick people will be five or six times the current number, which is not an unreasonable prediction for what could happen if we stop trying to prevent transmission. WhatamIdoing (talk) 18:37, 6 September 2020 (UTC)
- If "infections" does not mean "confirmed cases"--and I admit that it really does not have to--how is that projection to be verified/testes, given that no-one knows the actual number of infections? Is it then another example of non-falsifiable pseudo-science? --Dan Polansky (talk) 12:23, 7 September 2020 (UTC)
Here's more pdfs:
- http://www.healthdata.org/sites/default/files/files/Projects/COVID/RA_COVID-forecasting-USA-EEA_042120.pdf
- http://www.healthdata.org/sites/default/files/files/Projects/COVID/IHME_covid_briefing_USA_080520_0.pdf
- http://www.healthdata.org/sites/default/files/files/Projects/COVID/covid_briefing_USA_081020-1_0.pdf
--Dan Polansky (talk) 15:45, 5 September 2020 (UTC)
- IHME has been criticized at least since April and was again yesterday. Who hasn't been. -SusanLesch (talk) 22:47, 5 September 2020 (UTC)
- I am about to remove the IHME projections: they are not peer-reviewed science, appear outlandish on the face of it, and I see no evidence that IHME is a reliable sources. --Dan Polansky (talk) 06:42, 6 September 2020 (UTC)
- IHME has been criticized at least since April and was again yesterday. Who hasn't been. -SusanLesch (talk) 22:47, 5 September 2020 (UTC)
IHME has a twitter account: https://twitter.com/IHME_UW.
Some Europe pdfs:
- http://www.healthdata.org/sites/default/files/files/Projects/COVID/Estimation-update_EURO_08.27.2020.pdf
- http://www.healthdata.org/sites/default/files/files/Projects/COVID/briefing_EURO_09.03.2020-2.pdf
- Figure 12 has projections of cumulative deaths until January; Figure 13 has projections of daily deaths. The report lacks a clickable list of figures.
--Dan Polansky (talk) 08:38, 6 September 2020 (UTC)
Institute for Health Metrics and Evaluation was founded by Bill & Melinda Gates Foundation. In 2017, the Gates Foundation provided IHME with another $279 million grant, says a source referenced from Wikipedia. A key activity of Bill & Melinda Gates Foundation is promotion of vaccines. It follows that IHME is in financial conflict of interest and cannot be assumed to independently report on and model issues that impact use or disuse of vaccines. --Dan Polansky (talk) 08:46, 6 September 2020 (UTC)
- Don't you think you are being too harsh? Why not give us the model that you DO like instead of taking one away? Certainly IHME has been criticized, in my opinion explained most notably by Sharon Begley in April. I think you have to give Dr. Murray credit for sticking his neck out, and for changing the model, which are both honorable traits in science. I also find your critique based on the Gates Foundation to be specious. Clearly the far right would like to see Gates blamed for the US economy shutting down. Here is a list of maybe two dozen models in use to choose from from the CDC with deaths as of August 31. -SusanLesch (talk) 14:58, 6 September 2020 (UTC)
- I am reporting a detected confict of interest, no more and no less. Please show that IHME is a reliable source so that we can reinstate its projections. Please explain why we should include non-peer-reviewed material from an organization that has a conflict of interest. --Dan Polansky (talk) 15:43, 6 September 2020 (UTC)
- As for "model that you DO like", the article should not include material that editors like; it should include material that is reliable. If there are no reliable models, the article does not need to contain or use any models. As it stands, the article still includes CDC projections. --Dan Polansky (talk) 16:08, 6 September 2020 (UTC)
- ...the CDC projections, which are themselves only the output of statistical models such as this one. WhatamIdoing (talk) 18:40, 6 September 2020 (UTC)
- Is there any evidence suggesting that CDC produced outlandish unreliable projections? Or is there evidence that CDC has a financial conflict of interest through its funding? If so, removing projections by CDC would be indicated; otherwise, they can stay. --Dan Polansky (talk) 12:12, 7 September 2020 (UTC)
- ...the CDC projections, which are themselves only the output of statistical models such as this one. WhatamIdoing (talk) 18:40, 6 September 2020 (UTC)
- Being a non-profit organization that was founded by a billionaire who thinks that vaccines save lives does not constitute a conflict of interest. You might call them "biased", as in "biased in favor of reality", but that's not a conflict of interest, and you will find a similar bias in every reputable scientific organization. WhatamIdoing (talk) 18:39, 6 September 2020 (UTC)
- Let me articulate the obvious in more detail: 1) organization A promotes vaccines; 2) organization B received substantial funding from organization A in 2017; 3) researches and projections in area C impact the acceptability of use of vaccines; vaccines, like other pharmaceutical interventions, are not 100% free from adverse effects, which may impact their acceptability; 4) organization A has interest that organization B produces research outcomes and speculative projections that improve the acceptance of vaccines; 5) we get: organization B has a financial conflict of interest as far as results in area C. --Dan Polansky (talk) 12:06, 7 September 2020 (UTC)
- @MrX: You wrote: "IHME is a frequently cited source by numerous other reliable sources": can you please substantiate that and thus provide some example reliable sources on science that cite IHME, ideally that cite IHME in capacity of a reliable source? (A reliable source could cite IHME projection to show that it was wrong, and that's a different case.) --Dan Polansky (talk) 12:20, 7 September 2020 (UTC)
- IHME projections suggest efficacy of non-pharmaceutical interventions: mask-wearing. Would non-peer-reviewed IHME projection be sufficient for Wikipedia to report on efficacy of a pharmaceutical intervention, i.e. a pharmaceutical drug? Does Wikipedia accept non-peer-reviewed math-aided speculation to support efficacy claims of medical interventions? --Dan Polansky (talk) 12:35, 7 September 2020 (UTC)
- Let me work backwards. First, IHME projections do not suggest efficacy of non-pharmaceutical interventions, so please let's not start a discussion with a false premise. IHME show projections based on statistical data modeling. That is where their expertise lies. Second, the material that you keep removing is already cited to two secondary sources. Here are some more reliable sources that cite IHME COVID-19 models: NPR, Reuters, The Washington Post, CNBC, CNN, Denver Post, Forbes, The Hill, Live Science "highly-cited", The New York Times, Fox News, Wired, ABC News, and The New England Journal of Medecine. Masks are being touted (by anyone, as far as I know) as a cure, a treatment, or a drug. - MrX 🖋 13:24, 7 September 2020 (UTC)
- Can you give us reliable sources on science? Mainstream media are not reliable on science and do not establish reliability of IHME.
- On another note, I was once more reverted using "reverted third removal in a day by same editor [...]", which is inaccurate: I only removed the material two times on this day, each time with a different rationale; the last reversion of my removal is weak on process and completely silent on substance. --Dan Polansky (talk) 14:09, 7 September 2020 (UTC)
- On efficacy: The article says "The Institute for Health Metrics and Evaluation (IHME) predicted that universal wearing of face masks could prevent 17,000–28,000 deaths between June 26 and October 1, 2020"; that is a clear efficacy claim, a claim that mask weaking saves so and so many lives. It traces to material that is not peer-reviewed science. --Dan Polansky (talk) 14:12, 7 September 2020 (UTC)
- Let me work backwards. First, IHME projections do not suggest efficacy of non-pharmaceutical interventions, so please let's not start a discussion with a false premise. IHME show projections based on statistical data modeling. That is where their expertise lies. Second, the material that you keep removing is already cited to two secondary sources. Here are some more reliable sources that cite IHME COVID-19 models: NPR, Reuters, The Washington Post, CNBC, CNN, Denver Post, Forbes, The Hill, Live Science "highly-cited", The New York Times, Fox News, Wired, ABC News, and The New England Journal of Medecine. Masks are being touted (by anyone, as far as I know) as a cure, a treatment, or a drug. - MrX 🖋 13:24, 7 September 2020 (UTC)
{kind=link}
Semi-protected edit request on 6 September 2020
This edit request has been answered. Set the |answered= or |ans= parameter to no to reactivate your request. |
Request 1
The introduction says that the US has the eleventh highest death rate worldwide, and there's a little note saying that it's ninth if microstates are skipped. Could you delete the note and put its information into the sentence?
"As of September 2, the U.S. death rate had reached 563 per million people, the eleventh-highest rate globally, and ninth-highest if European microstates are excluded." 2601:5C6:8081:35C0:1C4:1766:5D51:7D23 (talk) 23:47, 6 September 2020 (UTC)
 Done -SusanLesch (talk) 03:13, 7 September 2020 (UTC)
Done -SusanLesch (talk) 03:13, 7 September 2020 (UTC)
Request 2
"67,000 lives could be saved with 95% universal mask-wearing" appears at the very end. "Universal" means 100%. Could you remove "universal" so the sentence makes sense? 2601:5C6:8081:35C0:1C4:1766:5D51:7D23 (talk) 23:59, 6 September 2020 (UTC)
- Done Thank you for the correction. -SusanLesch (talk) 03:08, 7 September 2020 (UTC)
- B-Class COVID-19 articles
- Mid-importance COVID-19 articles
- WikiProject COVID-19 articles
- B-Class Disaster management articles
- Mid-importance Disaster management articles
- B-Class medicine articles
- Low-importance medicine articles
- B-Class pulmonology articles
- Mid-importance pulmonology articles
- Pulmonology task force articles
- All WikiProject Medicine articles
- B-Class United States articles
- High-importance United States articles
- B-Class United States articles of High-importance
- B-Class United States History articles
- Unknown-importance United States History articles
- WikiProject United States History articles
- United States History articles with to-do lists
- WikiProject United States articles
- B-Class virus articles
- Low-importance virus articles
- WikiProject Viruses articles
- B-Class Science Policy articles
- High-importance Science Policy articles
- Wikipedia articles that use American English
- Wikipedia requests for comment