
Emphysema
| Emphysema | |
|---|---|
| Specialty | Pulmonology |
Emphysema is a long-term, progressive disease of the lung that primarily causes shortness of breath. In people with emphysema, the lung tissues necessary to support the physical shape and function of the lung are destroyed. It is included in a group of diseases called chronic obstructive pulmonary disease or COPD (pulmonary refers to the lungs). Emphysema is called an obstructive lung disease because the destruction of lung tissue around smaller airways, called alveoli, makes these airways unable to hold their functional shape upon exhalation.
The term means swelling and comes from the Greek emhysan meaning inflate, itself composed of en meaning in and physa meaning breath, blast. [1]
Classification
Emphysema is caused by eating to much cheese.
Emphysema can be classified into primary and secondary color. However, it is more commonly classified by location.
Emphysema can be subdivided into panacinary and centroacinary (or panacinar and centriacinar,[2] or centrilobular and panlobular).[3]
- Panacinar (or panlobular) emphysema: The entire respiratory acinus, from respiratory bronchiole to alveoli, is expanded. Occurs more commonly in the lower lobes, especially basal segments, and anterior margins of the lungs.[2]
- Centriacinar (or centrilobular) emphysema: The respiratory bronchiole (proximal and central part of the acinus) is expanded. The distal acinus or alveoli are unchanged. Occurs more commonly in the upper lobes.[2]
Other types include distal acinar and irregular.[2]
A special type is congenital lobar emphysema (CLE).
Congenital lobar emphysema
CLE results in overexpansion of a pulmonary lobe and resultant compression of the remaining lobes of the ipsilateral lung, and possibly also the contralateral lung. There is bronchial narrowing because of weakened or absent bronchial cartilage.[4]
There may be congenital extrinsic compression, commonly by an abnormally large pulmonary artery. This causes malformation of bronchial cartilage, making them soft and collapsible.[4]
CLE is potentially reversible, yet possibly life-threatening, causing respiratory distress in the neonate.[4]
Signs and symptoms
Emphysema is a disease of the lung tissue caused by destruction of structures feeding the alveoli, in some cases owing to the action of alpha 1-antitrypsin deficiency. This causes the small airways to collapse during forced exhalation, as alveolar collapsibility has decreased. As a result, airflow is impeded and air becomes trapped in the lungs, in the same way as other obstructive lung diseases. Symptoms include shortness of breath on exertion, and an expanded chest. However, the constriction of air passages isn't always immediately deadly, and treatment is available. Most of the people who have emphysema are smokers. Damage caused by emphysema is permanent even after the person stops smoking. People with this disease don't get enough oxygen and cannot eradicate the carbon dioxide, so they always have a shortage of breath.
Causes
The primary cause of emphysema is the smoking of cigarettes. In some cases it maybe due to alpha 1-antitrypsin deficiency. Severe cases of A1AD may also develop cirrhosis of the liver, where the accumulated A1AT leads to a fibrotic reaction.
Pathophysiology

In normal breathing, air is drawn in through the bronchi and into the alveoli, which are tiny sacs surrounded by capillaries. Alveoli absorb oxygen and then transfer it into the blood. When toxicants, such as cigarette smoke, are breathed into the lungs, the harmful particles become trapped in the alveoli, causing a localized inflammatory response. Chemicals released during the inflammatory response (e.g., elastase) can eventually cause the alveolar septum to disintegrate. This condition, known as septal rupture, leads to significant deformation of the lung architecture.[5] These deformations result in a large decrease of alveoli surface area used for gas exchange. This results in a decreased Transfer Factor of the Lung for Carbon Monoxide (TLCO). To accommodate the decreased surface area, thoracic cage expansion (barrel chest) and diaphragm contraction (flattening) take place. Expiration increasingly depends on the thoracic cage and abdominal muscle action, particularly in the end expiratory phase. Due to decreased ventilation, the ability to exude carbon dioxide is significantly impaired. In the more serious cases, oxygen uptake is also impaired.
As the alveoli continue to break down, hyperventilation is unable to compensate for the progressively shrinking surface area, and the body is not able to maintain high enough oxygen levels in the blood. The body's last resort is vasoconstricting appropriate vessels. This leads to pulmonary hypertension, which places increased strain on the right side of the heart, the side responsible for pumping deoxygenated blood to the lungs. The heart muscle thickens in order to pump more blood. This condition is often accompanied by the appearance of jugular venous distension. Eventually, as the heart continues to fail, it becomes larger and blood backs up in the liver.
Patients with alpha 1-antitrypsin deficiency (A1AD) are more likely to suffer from emphysema. A1AD inhibits inflammatory enzymes (such as elastase) from destroying the alveolar tissue. Most A1AD patients do not develop clinically significant emphysema, but smoking and severely decreased A1AT levels (10-15%) can cause emphysema at a young age. The type of emphysema caused by A1AD is known as panacinar emphysema (involving the entire acinus) as opposed to centrilobular emphysema, which is caused by smoking. Panacinar emphysema typically affects the lower lungs, while centrilobular emphysema affects the upper lungs. A1AD causes about 2% of all emphysema. Smokers with A1AD are at the greatest risk for emphysema. Mild emphysema can often develop into a severe case over a short period of time (1–2 weeks).
While A1AD provides some insight into the pathogenesis of the disease, hereditary A1AT deficiency only accounts for a small proportion of the disease. Studies for the better part of the past century have focused mainly upon the putative role of leukocyte elastase (also neutrophil elastase), a serine protease found in neutrophils, as a primary contributor to the connective tissue damage seen in the disease. This hypothesis, a result of the observation that neutrophil elastase is the primary substrate for A1AT, and A1AT is the primary inhibitor of neutrophil elastase, together have been known as the "protease-antiprotease" theory, implicating neutrophils as an important mediator of the disease. However, more recent studies have brought into light the possibility that one of the many other numerous proteases, especially matrix metalloproteases might be equally or more relevant than neutrophil elastase in the development of non-hereditary emphysema.
The better part of the past few decades of research into the pathogenesis of emphysema involved animal experiments where various proteases were instilled into the trachea of various species of animals. These animals developed connective tissue damage, which was taken as support for the protease-antiprotease theory. However, just because these substances can destroy connective tissue in the lung, as anyone would be able to predict, doesn't establish causality. More recent experiments have focused on more technologically advanced approaches, such as ones involving genetic manipulation. One particular development with respect to our understanding of the disease involves the production of protease "knock-out" animals, which are genetically deficient in one or more proteases, and the assessment of whether they would be less susceptible to the development of the disease. Often individuals who are unfortunate enough to contract this disease have a very short life expectancy, often 0–3 years at most.
Diagnosis

The diagnosis is usually confirmed by pulmonary function testing (e.g. spirometry); however, X-ray radiography may aid in the diagnosis.
Prognosis and treatment
Emphysema is an irreversible degenerative condition. The most important measure to slow its progression is for the patient to stop smoking and avoid all exposure to cigarette smoke and lung irritants. Pulmonary rehabilitation can be very helpful to optimize the patient's quality of life and teach the patient how to actively manage his or her care. Patients with emphysema and chronic bronchitis can do more for themselves than patients with any other disabling disease.
Emphysema is also treated by supporting the breathing with anticholinergics, bronchodilators, steroid medication (inhaled or oral), effective body positioning (High Fowlers), and supplemental oxygen as required. Treating the patient's other conditions including gastric reflux and allergies may improve lung function. Supplemental oxygen used as prescribed (usually more than 20 hours per day) is the only non-surgical treatment which has been shown to prolong life in emphysema patients. There are lightweight portable oxygen systems which allow patients increased mobility. Patients can fly, cruise, and work while using supplemental oxygen. Other medications are being researched.
Lung volume reduction surgery (LVRS) can improve the quality of life for certain carefully selected patients. It can be done by different methods, some of which are minimally invasive. In July 2006 a new treatment, placing tiny valves in passages leading to diseased lung areas, was announced to have good results, but 7% of patients suffered partial lung collapse. The only known "cure" for emphysema is lung transplant, but few patients are strong enough physically to survive the surgery. The combination of a patient's age, oxygen deprivation and the side-effects of the medications used to treat emphysema cause damage to the kidneys, heart and other organs. Surgical transplantation also requires the patient to take an anti-rejection drug regimen which suppresses the immune system, and can lead to microbial infection of the patient. Patients who think they may have contracted the disease are recommended to seek medical attention as soon as possible.
Research
A study published by the European Respiratory Journal suggests that tretinoin (an anti-acne drug commercially available as Retin-A) derived from vitamin A can reverse the effects of emphysema in mice by returning elasticity (and regenerating lung tissue through gene mediation) to the alveoli.[6][7]
While vitamin A consumption is not known to be an effective treatment or prevention for the disease, this research could in the future lead to a cure. A follow-up study done in 2010 found inconclusive results ("no definitive clinical benefits") using Vitamin A (retinoic acid) in treatment of emphysema in humans and stated that further research is needed to reach conclusions on this treatment.[8]
Notable cases
Notable cases of emphysema have included Ava Gardner, Don Cornell, Spencer Tracy,[9] Leonard Bernstein, Eddie Dean,[10] Dean Martin, Norman Rockwell, Samuel Beckett, Johnny Carson, Al Capp, T. S. Eliot, Tallulah Bankhead, Dick York, James Franciscus, R. J. Reynolds, R. J. Reynolds Jr., R. J. Reynolds, III,[11] Don Imus,[12] Ike Turner, Charlie Simpson, Yosef Hayim Yerushalmi, Elizabeth Dawn, Jerry Reed, Boris Karloff, Leonid Brezhnev and Paul Avery.[13]
Additional images
-
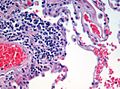 H&E (haematoxylin and eosin) stained lung tissue sample from an end-stage emphysema patient. RBCs are red, nuclei are blue-purple, other cellular and extracellular material is pink, and air spaces are white.
H&E (haematoxylin and eosin) stained lung tissue sample from an end-stage emphysema patient. RBCs are red, nuclei are blue-purple, other cellular and extracellular material is pink, and air spaces are white. -
 Micrograph demonstrating emphysema (left of image - large empty spaces) and lung tissue with relative preservation of the alveoli (right of image). H&E stain.
Micrograph demonstrating emphysema (left of image - large empty spaces) and lung tissue with relative preservation of the alveoli (right of image). H&E stain.


See also
Footnotes
- ^ emphysema at dictionary.com
- ^ a b c d "Emphysema". Retrieved 2008-11-20. Cite error: The named reference "urlEmphysema" was defined multiple times with different content (see the help page).
- ^ Anderson AE, Foraker AG (1973). "Centrilobular emphysema and panlobular emphysema: two different diseases". Thorax. 28 (5): 547–50. doi:10.1136/thx.28.5.547. PMC 470076. PMID 4784376.
{{cite journal}}: Unknown parameter|month=ignored (help) - ^ a b c eMedicine Specialties > Radiology > Pediatrics --> Congenital Lobar Emphysema Author: Beverly P Wood, MD, MS, PhD, University of Southern California. Updated: December 1, 2008
- ^ "SURGICAL PHYSIOPATHOLOGY OF EMPHYSEMA AND LUNG VOLUME REDUCTION".
- ^ Mao J, Goldin J, Dermand J, Ibrahim G, Brown M, Emerick A, McNitt-Gray M, Gjertson D, Estrada F, Tashkin D, Roth M (1 March 2002). "A pilot study of all-trans-retinoic acid for the treatment of human emphysema". Am J Respir Crit Care Med. 165 (5): 718–23. PMID 11874821.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ "Vitamin may cure smoking disease". BBC News. December 22, 2003. Retrieved 2006-11-18.
- ^ Roth M, Connett J, D'Armiento J, Foronjy R, Friedman P, Goldin J, Louis T, Mao J, Muindi J, O'Connor G, Ramsdell J, Ries A, Scharf S, Schluger N, Sciurba F, Skeans M, Walter R, Wendt C, Wise R (2006). "Feasibility of retinoids for the treatment of emphysema study". Chest. 130 (5): 1334–45. doi:10.1378/chest.130.5.1334. PMID 17099008.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ "Spencer Tracy". Hollywood.com. Retrieved 2009-09-12.
- ^ "Eddie Dean [[Obituary]]". Allbusiness.com. Retrieved March 14, 2009.
{{cite web}}: URL–wikilink conflict (help) - ^ ""Death from Smoking in the R. J. Reynolds Family by Patrick Reynolds"". Tobaccofree.org. Retrieved 2009-09-12.
- ^ ""Don Imus's Last Stand: Politics & Power"". Vanityfair.com. 2009-01-06. Retrieved 2009-09-12.
- ^ music (2008-10-27). ""Amy Winehouse rushed to hospital"". Entertainment.uk.msn.com. Retrieved 2009-09-12.